Material Shifts
Theorizing Endometriosis, Embodiment, and Experimental Art



1_Introduction [1]
As a writer, I have always found poetry and prose to be the most satisfying methods to work through my observations, ideas, and embodiment. But the language of the body — and its metaphors — has its own limitations. When grappling with illness bound up within the reproductive organs, words either reek of their clinical orientation or are flagrantly gendered or sexual. Certainly, the medical and the erotic make for good poetry: but the experience of being sick, and being examined over and over again, shifts embodiment itself. Physical exams require careful corporeal management, a studied calibration of when stoicism or expressions of pain are needed. Conversations with specialists demand talking points, make-up, and anti-anxiety medication. Phone calls with the physician are more comfortable, allowing space for my worry and skepticism. But at the end of each medical encounter, the body is still committed to its silent recording of each pinch, ache, and tear, documenting an internal scar that I imagine thickening over time. My reproductive organs have grown ropy as hard fists, punching their way out. I offer instead of those unwritten poems this article, framed around an experimental art-practice to reflect my shifting materiality.
Throughout this article, I reflect on incidences in the past year of my worsening pelvic health. Last summer, I noticed something in my pelvis felt distinctly off. Already prone to distinctive chronic pain and fatigue flares at multiple points in my menstrual cycle, I was disconcerted by a new problem that seemed to come out of nowhere. I have struggled with the symptoms of endometriosis, PTSD, anxiety, and depression for over twenty years, a grab-bag of chronic illnesses that exacerbate one another and require constant management and attention. My medical file, and my increasingly fragmented body, has bounced between as many specialists as years as I have sought a firm diagnosis of endometriosis. [2] While specialist after specialist has confirmed I have numerous endometriosis symptoms, I have struggled to find a specialist willing to undertake diagnostic surgery to confirm their suspicions. Instead, their advice was always the same: birth control, IUD, and chemical menopause. Two years ago, frustrated by the side effects of yet another failed birth control attempt — this time the lowest dose on the market — I swore to my general practitioner that I was giving up on gynecological interventions and would instead focus on non-invasive pain management strategies. This promise to myself, known also as ‘giving up hope,’ resulted in my withdrawal into my chronic illness with a sense of ambivalence. No more investigative exams, ultrasounds, hormones, or tests; I would just cope.
This plan was working well enough — I continued to mask my chronic illnesses as an adjunct professor and postdoctoral research fellow—until the recent shift occurred in my pelvis, alerting me that something else was wrong. No longer invisible, my uterus announced its discontent in an alarming way, demanding immediate specialist intervention. For once, it was not the cloudy shroud of endometriosis but a structural issue that was visible with the trained urogynecological eye: unexplained total pelvic prolapse. Without cause or warning, the muscles in my pelvis had weakened, releasing my reproductive organs from their hold. Since they were no longer in their right place, the specialist recommended the removal of my uterus through a reparative hysterectomy. Suddenly, my body required surgical intervention; I was finally sick enough to warrant medical care.
This material shift of my reproductive organs, and the attendant medical, theoretical, narrative, and artistic inquiries it inspired, form the shape of this autotheoretical article. [3] As queer theorist Eve Kosofsky Sedgwick observed of her own relationship with terminal illness and narrative, “the absolute privilege of the writing act itself” had to adjust to changes in bodily and affective capacities. [4] My experience of having to reconcile with a shifting embodiment required reimagining how to express the experience of illness, in particular when the chronic illness itself is signified as deeply gendered. [5] From the standpoint of my own observations as a white working-class queer academic worker, I first take an analytical approach to theorizing chronic illness, moving from a medical to a feminist disability lens to understand endometriosis symptoms. My discussion then turns towards finding a language for the affective dimensions of illness — pain, fatigue, anxiety, shame — that live deep within the body. What might it mean to use a creative arts-based practice to externalize these more private aspects of chronic illness? This question drives my inquiry into art as a mode of narrating chronic illness and disability. By examining how a disability aesthetic privileges and legitimizes non-normative embodiment, I consider how symptoms of endometriosis and chronic pelvic pain can be expressed outside of the medical gaze. Finally, I use my own experimental arts-based process to explore art as an alternative method for coping with and narrating chronic illness.
2_Defining Endometriosis in Medical Terms
Endometriosis is a progressive, incurable disease suspected of impacting 1 in 10 female-assigned people with uteruses, and is commonly understood as a menstrual disorder characterized by painful periods. [6] Endometriosis is caused by tissue that is similar to, but different from, the cells that develop the endometrium inside the uterus; however, endometriosis tissue corresponds to hormonal fluctuations, bleeds, and sheds outside of the uterus. [7] In dismissing abnormal menstrual pain and bleeding, doctors may then fail to identify the diseases’ lesions and adhesions that cover, fuse, or inhibit the normal functioning of pelvic organs. [8] As scholars and activists in the field of critical menstruation studies demonstrate, menstruation is a political process mediated by raced, classed, sexualized, and gendered access to resources, education, and healthcare. [9] The stigma associated with menstruation can limit both patients and doctors from investigating complaints of menstrual pain further. [10] Simultaneously, the validity of women and queer people’s assessment of their own experiences are often questioned by medical professionals. [11]
A misconception about endometriosis is that avoiding or postponing pregnancy can cause endometriosis to grow, charging cisgender women with reproduction as a disease preventative. [12] Indeed, known in the 1980s-90s as the “career women’s disease,” the marked incidence of endometriosis in white, middle-upper class professional women authorized a misogynist medical discourse that saw endometriosis as a punishment for these women forestalling their primary duty of motherhood. [13] While endometriosis has never been confined to this demographic, the race, class, gender, and sexuality of the patient constitute clinical perceptions of the disease. [14] At odds with a privileging of class-privileged white women’s fertility are the horrific incidences of forced sterilizations, gynecological experimentations, and refusals of care encountered by race, class, sexual, and gender minorities. [15] Notwithstanding that endometriosis causes infertility in approximately 30-40% of people impacted with the disease, reproduction does not provide a long-term prevention for the growth of endometriosis tissue. [16] However, preserving or rehabilitating fertility continues to be the primary goal of many surgeons, gynecologists, and primary care physicians, relegating pain, disability, and the loss of quality of life as secondary concerns. [17]
As this section has demonstrated, endometriosis is a “complex disease” prone to infiltrate, inflame, and interfere with broad systems of the body. [18] Beyond cisgender women’s reproductive organs, endometriosis cells have been found in every human organ besides the spleen, in cisgender men, and even in fetuses. [19] Endometriosis is characterized by a range of bodily symptoms that extend beyond dysmenorrhea and infertility, including weakness of breath, chronic fatigue, chronic pain, chronic anemia, and brain fog, rendering it a total body disease that is debilitating and disabling. [20] The stigma of menstruation, a lack of expert knowledge by medical practitioners, and the minimizing of women, racialized, poor, mentally ill, and gender-diverse people’s pain, results in endometriosis being under-diagnosed and grossly mismanaged. [21] The absence of a cure, the socio-economic barriers to treatment, and the overall impact of the disease on work, health, fertility, identity, and intimacy create a complex psychological burden. In the following section, I use a feminist disability framework to move endometriosis symptoms beyond the medical model of disease management.
3_Living With Endometriosis Symptoms: A Feminist Disability Studies Perspective
In Canada, endometriosis is not considered a disability. Reflecting this context, Canadian endometriosis advocates are working on a range of projects aimed to raise awareness of the disease. The Endometriosis Network Canada (TENC) is a not-for-profit organization that formed in 2012 to share resources and offer support to people with endometriosis. [22] It currently provides online support groups and a resource list of endometriosis specialists. Recently, Endometriosis Network Canada became trans and gender non-conforming inclusive. EndoAct Canada, an affiliate of TENC, is an organization led by advocates, patients, and health-care providers seeking to drive policy change. [23] EndoAct Canada is currently compiling stories from people with endometriosis across Canada in an effort to document the severity of the disease, the difficulty of obtaining a diagnosis, and the socio-economic indicators of health (race, class, sexuality, gender) that impact how endometriosis is experienced. Yet another project is #PrioritizePain, a public awareness campaign that corresponds to An Action Plan for Pain in Canada. [24] The Action Plan is the result of the 2019 Canadian Pain Task Force’s recommendation for broad-based policy change to proactively address the one in five Canadians experiencing chronic pain. These important projects work to legitimize endometriosis and chronic pain, and to transform the policies that structure care. But in their pursuit for improving care, they have left out the language of disability from the conversation.
In contrast, I argue for understanding endometriosis and endometriosis-like symptoms as a disability, acknowledging that disability justice seeks a transformation of all the power structures in society that relegate to the margins bodies that are non-normative. [25] Thinking about chronic illness as a disability is indebted to the pioneering work of Susan Wendell in the field of feminist disability studies. [26] Recognizing that the burgeoning social movement theories of feminism and disability had little overlap with one another, Wendell set out in 1989 to theorize disability in relation to racism, classism, and sexism. [27] Also taking as a starting point her own personal experience of disability through chronic illness, Wendell raised a series of considerations that destabilized taken-for-granted norms not only in medical discourse, but in both feminist and disability theory. These interventions contributed to the establishment of feminist disability studies as a legitimate field for examining sick and disabled embodiment. [28] More recently, Cara Jones has argued for a feminist disability studies framework for understanding endometriosis. [29] Jones’ project questions the silence around endometriosis in both feminist and disability studies writing on chronic illness, asking why such a wide-spread disease that predominantly affects people assigned female at birth (AFAB) has been so under-examined. To Jones, a heteronormative reading of endometriosis as ‘female problems’ that at worst impact fertility ignores the complex, disabling, and isolating effects of pain associated with the condition. [30] Jones claims that “biopsychosocial pain is the major issue for those with endometriosis: the lived experience of pain, its social context, and the ways it is interpreted.” [31] A feminist disability lens resists the individualization of pain and situates it within the social world.
Endometriosis and endometriosis-like symptoms are disabling; like other chronic illnesses, bodily symptoms “cannot be eliminated, perhaps not even mitigated, by social arrangements.” [32] For instance, one aspect of chronic illness as a disability is the unpredictability of managing symptoms. While having access to a non-gendered private and accessible bathroom in public or at work may be helpful, a pain or bleeding flare may necessitate staying home in close proximity to one’s own bathroom and pain management tools (heating pads, ice packs, compression socks, face mask, ear plugs, pain killers, etc.). [33] The unpredictability of the timing and the severity of a pain flare impacts navigating all aspects of the social world. Chronic pain forms a backdrop to life, drawing a ring around what is possible. [34] Despite the fact that nothing will cure the disease or even necessarily lessen the intensity or frequency of the pain, people with endometriosis-like symptoms are routinely proscribed a careful regime of self-management. [35] Individuals are held responsible—by doctors and employers, and often family and friends—for staying on top of symptoms, causing anxiety, grief, and shame for the unpredictability of the body.
In the cases where surgery to excise endometriosis tissue is feasible, affordable, and accessible, surgery may lessen, but rarely alleviate, chronic pain. [36] However, even obtaining a diagnosis, let alone treatment, is a significant barrier amongst many people with endometriosis symptoms. [37] In the Western world, it takes from eight to ten years on average to receive a diagnosis of endometriosis. [38] What this statistic does not reveal are the countless doctors and specialists who, in the interim, discount, disregard, and deny existence of the disease. [39] Establishing a diagnosis for a condition that requires advanced ultrasound and laparoscopic surgery to identify requires multiple levels of medical care, a scenario out of reach for many. [40] In particular, those who are rural, low-income, racialized, trans, and queer face additional barriers to receiving specialist attention. Moreover, a history of mental illness or drug use can also occlude medical perspectives, chocking up chronic pain as ‘in the head’ or a plea for opioids.
Endometriosis diagnosis can affirm a sense of suffering and operationalize a treatment plan. Diagnosis can enable appropriate pain management, surgery, physiotherapy, and for those who seek it, fertility resources. Relying on others for care is a common strategy of living with chronic illness, and diagnosis can also legitimize experience, encouraging support from co-workers, family, and friends. [41] Diagnosis can also encourage participation in support groups, both in-person and online. [42] Online support groups offer a counter to the isolation of disease, provide insider tips on treatment side effects, and empower individuals to be more active in their doctor-patient relationships. The wait for a diagnosis is so fundamental to the disease that the endometriosis community, at least digitally, is very welcoming of members at every stage of their journey. Anecdotally, I have observed how hetero-normative concerns and outcomes (fertility, dyspareunia) rank on par with pain, medication, hormones, and surgery as key sources of discussion. Not surprisingly given the medical approach to endometriosis, pelvic pain, and reproductive health more generally, conversations around endometriosis as a disability occur more sparingly. As noted above, the lack of a disability analysis within endometriosis advocacy organizations may contribute to this.
For people like me, surgical diagnosis might provide access to disability accommodations and employment equity resources from within my institutions. [43] In my experience in academia, as both a graduate student and an adjunct professor, I must self-identify as disabled in formal and informal ways in order to access these protections. [44] As each of my chronic illnesses are invisible, I have historically chosen ‘to pass’ as healthy, granting me both privileges from discrimination while also prohibiting my access to various accommodations in the university. [45] Part of my decision to previously mask my illnesses has been a fear of stigma, discrimination, and potential loss of employment, opportunity, and trust. [46] These fears reveal the internalized ableism that comes from being in an environment that distinctly rewards exceptionalism, individualism, and independence—the very ideals that feminist disability studies has critiqued. Indeed, in accommodating chronic illness, the university, as many other institutions and labour relations, is bound by two competing ideologies: disability protections that guarantee equal access and participation, versus a highly hierarchical ethos of competitive productivity. [47] Experiencing chronic illness often means navigating chronic fatigue and chronic pain, resulting in complex needs for accommodation of “pace and flexibility about time” that disrupt neoliberal and capitalist notions of productivity. [48]
Accommodating chronic illness at all levels of work in the academy remains an urgent issue for feminist disability justice, particularly because chronic illnesses overwhelmingly affect cisgender women. [49] While recent research on chronic illness in Canadian universities has demonstrated positive outcomes of employment retention for academic workers who experienced disability after obtaining a permanent position, being sick and disabled prior to employment is another story. [50] In the first place, professorship is an extremely coveted position, with only 20% of PhD graduates landing in an academic job. [51] Even prior to that, structural and individual forms of discrimination — racism, classism, sexism, ableism, homophobia, whorephobia, transphobia — all inflect an individual’s trajectory in academia. Similarly, these same biases impact student experiences of the institution, demonstrated by the high levels of scrutiny and distrust female-identified students encounter when seeking accommodations. [52] All this is to say that to identify oneself as disabled within academia, in particular for chronic illness sufferers, is a highly personal, precarious, and strategic undertaking.
To experience chronic illness has material consequences on access not only to educational or employment accommodations, but to income support when employment is no longer possible, in the short or long term. Yet how chronic illnesses, particularly those that disproportionately affect women, are constructed in income support discourse is critical to combating the correlation between disability and poverty. [53] For instance, the DisAbled Women’s Network of Canada (DAWN) reports that despite the higher incidence of chronic illness and chronic pain amongst women, employment insurance is less likely to support these conditions than more visible forms of workplace injury. [54] DAWN states further that, “for those with episodic disabilities there are additional barriers to qualifying for provincial and national income security systems as definitions of disability often rely on being either fully disabled or fully able to work which leads to conditions that make poverty more prevalent.” [55] As research demonstrates, women who experience chronic illness are regularly denied access to provincial disability support for being “not disabled enough.” [56] For those who are deemed eligible for support, the poverty-level payments ensure low-income disabled and chronically ill women remain economically, socially, and physically marginalized. [57] For low-income women who experience chronic illness and disability, poverty is a very likely outcome. [58]
These issues reflect my own experience. Prior to obtaining funding for my doctoral research, I had always lived in varying states of poverty, including completing my high school diploma on social assistance. Pursuing higher education and academia has been my only path towards white-collar work. Throughout my degrees, I have been able to mask my invisible illnesses because of how private, unstandardized, and solitary academic work is. My white privilege and conventional femininity also contributed to this ease. At the same time, I juggled being poor, queer, and a trauma survivor in a white, wealthy, heteronormative space. Despite confiding in a select few mentors and friends along the way, I kept the extent of my illnesses from my students, peers, and professors. Even through my first semester of teaching full-time while I waited for my postdoctoral fellowship to begin, I managed my symptoms and fatigue with the kinds of subtle accommodations I routinely made for myself, including sitting down while lecturing with a hot-water bottle on my lap. However, when my health got worse this summer, it became clear that in future I would need to be more upfront about my illnesses, not only with my new research supervisor or my students, but also with myself. Telling my mentor about my recent condition was stressful, but it was also liberating; feminist disability studies has given me the language to do this. [59]
There are many structural barriers to supporting precarious academic workers with chronic illness—including permanent work and health benefits. For instance, as a current postdoctoral fellow, my income is taxable but is not eligible for employment insurance. What this means is that if I take a medical leave for pain, fatigue, or surgery, I will be unpaid and ineligible for government support. This system relies on the safety net of class privilege to make up for institutional failures to accommodate disability, illness, and chronic pain. For poor and working-class people in the university, to be sick is a liability. To me, poverty is not an abstract concept but a shadow that haunts me, burrowed deep into my cells. My biggest fear throughout academia has been to be discovered as the imposter I truly am, my potential grasp on a middle-class income forever snatched away. I desperately want the financial security that enables me to take care of myself, not only in spite of the work I do, but in order to do that work well. What kind of life might I lead if I allow chronic illness to take its rightful place in my narrative? And where my words shy away from articulating the more private details of my illness, will art take up that task? In the following section, I turn to a discussion of the politics of art, disability, and illness in order to contextualize my own experimental art practice.
4_Art and Illness, Disability, and Endometriosis
This summer, as my body intensified its disapproval of my reproductive organs, I felt a need to make sense out of what was happening in a way that felt physical. No longer satisfied by the roundness of words or the sharpness of syllables in my poetry, I wanted to feel something different. Sedgwick also found a similar need, as her terminal breast cancer demanded an unwelcome reckoning with her embodiment. Long hailed as the founder of queer theory with a wonderfully non-identitarian approach to the body, Sedgwick grappled with a means to express her experience outside of language. Turning towards textile art, Sedgwick discovered a way of articulating thoughts to feelings that relied upon touch. She wrote,
Even more immediate than other perceptual systems, it seems, the sense of touch makes nonsense out of the dualistic understanding of agency and passivity; to touch is always already to reach out, to fondle, to heft, to tap, or to enfold, and always also to understand other people or natural forces as having effectually done so before oneself, if only in the making of the textured object. [60]
Illness dissolves the boundary between agency and passivity. In my experience, illness upsets any coherent binary between the mind and the body, movement and stasis, choice and force; anyone who has been bed-ridden knows this well. [61] By shifting attention to touch as sense, it is not only the body that is being touched — painfully, comfortingly, invasively — but that is touching other spaces, shapes, structures. And when done so through the mediation of material sculpture, this practice of art making — as a form of touch — becomes a relation. The body is no longer perceived as siloed in illness, but as engaged throughillness.
The textile artist Judith Scott is the artistic subject of Sedgwick’s (final) book cover. A source of inspiration for Sedgwick’s own experimentation in textiles, Scott is renowned for her fiber-based sculpture practice of wrapping and binding different objects together into brightly colored amorphous structures. [62] What has been considered most exceptional about Scott’s story is that she came into her artistry after spending the majority of her life institutionalized for having Down’s Syndrome. When her twin sister attained stewardship over Scott, Scott was enrolled in the Creative Growth Center in Oakland, California, an arts program for persons with developmental, intellectual, and physical disabilities. It was in this artist-run program that Scott developed her art, and in turn, new modes of expression and communication, including her own personal style. [63] As Canadian art critic Luanne Martineau asserts, Scott’s impressive practice and body of work reveals that “there are different ways of knowing.” [64] Scott’s work attests to the various registers of feeling and touch that demand a reckoning beyond language.
In another assessment of the critical importance of Scott’s work, Tobin Siebers offers that disability is an aesthetic in its own right. [65] Rather than lament a lack of positive representation of disability in art, Siebers argues that images of the disabled body and mind have in fact been intrinsic to the development of aesthetic values. [66] In Siebers’ view, disability aesthetics have long been doing the work to make art more human and humane; to operationalize disability aesthetics is to recognize the possibility that disability provokes. He argues,
Disability aesthetics prizes physical and mental difference as a significant value in itself. It does not embrace an aesthetic taste that defines harmony, bodily integrity, and health as standards of beauty. Nor does it support the aversion to disability required by traditional conceptions of human or social perfection. Rather, it drives forward the appreciation of disability found throughout modern and avant-garde art by raising an objection to aesthetic standards and tastes that exclude people with disabilities. [67]
To Siebers, disability aesthetics provide a framework for resisting normativity and proliferating difference. It is a mode to resist not only the judgments of what qualifies as good art, but what qualifies as a good life. A disability aesthetic inherently values the disabled and chronically ill, assigning intrinsic meaning to artwork produced through, by, from, or about disabled embodiment.
Art can be a therapeutic way of coping with a changed or changing subjectivity. [68] Art as a form of therapy emerged in North America in the 1940s, reaching its heyday in the 1960s with the publication of Bulletin of Art Therapy. [69] This was followed by a new methodology, Arts Based Research (ABR), which sought to include arts-based practices within qualitative research projects. [70] ABR allows both researchers and their participants to engage with modalities outside of language, facilitating different kinds of information and relations (creating individual or group art, writing, film, installations, etc.) beyond the standard methods of qualitative study (surveys, focus groups, participant observation, etc.). [71] When taken up in the humanities and social sciences, arts based research at best “allows a sensory, bodily engagement with the research endeavor.” [72] This framework is useful for tapping into how disability, mental illness, and chronic illness are experienced and managed through artistic expression. [73] For instance, some women experiencing shifts in their identities and energy due to chronic illness and disability report that making art can be both a new discovery and something that is no longer a possibility. [74] At the same time, neither therapy nor academic research has historically been safe spaces for disabled, mad, and chronically ill women. [75] There is a risk that Arts Based Research and Art Therapy imagine disability and chronic illness as in need of therapeutic interventions, reinforcing a medical model of disability as an individual problem needing to be fixed. [76] However, a feminist disability studies lens can allow for the utility of arts-based practice as a mode of self-discovery, self-actualization, and self-regulation that is not a solution to disability and chronic illness, but one tool among many to process and communicate the experience.
For those with endometriosis and associated symptoms — including depression, anxiety, fatigue, and cyclical pain — arts-based practices can offer a way to make meaning from illness. Furthermore, as diseases relating to female-assigned reproductive organs are laden with assumptions, art can provide counter-narratives to medical discourse. For instance, Ellie Kammer, an Australian artist, depicts women’s experiences of endometriosis in larger-than-life oil paintings. [77] Kammer’s paintings maintain a formalistic approach to the Western ideal of feminine beauty, displaying cisgender women — typically white — in varying positions of lounging or recline. However, Kammer disrupts the viewers’ gaze with shades of red strewn across their abdomens, shadows of the reproductive organs beneath it. Red paint is also slashed onto her subjects’ thighs. Kammer describes her art as a way to challenge “the general ignorance surrounding the disease” and to affirm the experience of those with endometriosis. [78] In acknowledging the havoc endometriosis can inflict on one’s sense of embodiment, Kammer extends an invitation of self-acceptance towards others grappling with pain and illness.
In one sense, Kammer’s work joins a history of women making art about menstruation. [79] Menstrual art emerged as a genre in the second-wave women’s movement when feminist artists — like Judy Chicago — created images and installations using menstruation as their primary subject. [80] Contemporary artists continue to examine the politics of menstruation and its impact on embodiment in a variety of forms. [81] However, while menstruation and its attendant symptoms can be difficult to endure in general, it is disordered menstruation that is of interest to Kammer and to this inquiry here. In situating non-normative menstruation within a feminist disability framework, it becomes clear how some experiences of menstruation are in fact disabling. A disability aesthetic launches an inquiry into what forms of art are expected to do. For instance, art that exposes menstruation as taboo is certainly useful for thinking about gendered inequality. [82] More significantly for this discussion, art that locates menstruation as an aspect or cause of disability asks what non-normative menstruation might mean, expanding representation of non-normative gendered embodiment more generally. [83] It is to my own experimentation with an arts-based practice for narrating illness that I now turn.
5_Experimenting with Textile Representation of Illness
When I was first diagnosed with anxiety, depression, and PTSD, I was seventeen years old. I had left home a year prior and after a year on my own, moved into a group home for teenagers with mental health issues where I could get support. I recall this time as marked by the solace I would find as my pen hit the pages of my notebook, furiously scribbling poetry or journaling. But in the care of the group home a therapist was assigned to me, and we had weekly sessions that began using Art Therapy as method for trauma counselling. In these sessions with my therapist, I drew, colored, and played with clay; back at the group home, I was a bit more erratic, breaking things or tearing up whole books page by page. As Sedgwick suggests, “a particular intimacy seems to subsist between textures and emotions.” [84] There was something distinctly satisfying about the feeling of using my hands in creating or destroying objects; art provided a method of accessing affect that had been hard to reach for within language. With the support of my youth worker, I began painting, the staff supportive and providing me with materials and encouragement. Using acrylic paint on large canvases, I made abstract images that reflected the fear, anger, and sadness that plagued me. Bold reds, blacks, greens, yellows, and blues dominated in overlapping rectangles, squares, and lines. Instead of the soft tip of the paintbrush, I experimented with applying paint using its wooden tip. I moved on to rulers, cardboard, string, eventually preferring a kind of DIY printmaking to actual strokes of the brush on canvas. Up close, I mixed water and colors, rotating the canvas to control bleeding. The paintings took me multiple evenings to complete, and were a welcome distraction from the more destructive coping mechanisms I practiced. Later that year, the youth service held an art show for its residents, and all of my friends came to the opening. A local newspaper published a photo of me in front of my piece; I don’t have any of those paintings anymore.
Twenty years later, and with a second poetry manuscript out for review, I again found myself craving something besides words. One part of this story is the way in which PTSD from sexual violence impacts my health. Last summer, triggered by a reminder of a traumatic experience, I got very sick. My anxiety and depression skyrocketed, my body ached painfully, and my endometriosis symptoms worsened. I tried to access talk therapy, but was put on a six-month wait list for counseling at the local rape crisis center. When my uterus and bladder prolapsed that same month, I felt betrayed by my body, like it was refusing to let me move on from the feelings of the assault. I perceived that all the strides I had made in coping with my symptoms were crashing around me as I was overcome with the memories and the panic of yet another issue in my reproductive organs. This would mean more doctors, more examinations, more uncertainty, more diagnoses.
These three images below (Fig. 1-3) are textiles that represent different moments of experiencing my chronic illnesses, brought on by the events of last year. While lying in a dark room with a migraine, body aches, and pelvic cramping, while the sun blazed on outside, I visualized a meditative act of stitching together bright colors and soft cotton. Hours spent in bed unable to read, watch TV, or look at my phone turned into planning out how to achieve this art project. The method unfolded: bolts of fabric, pinks and purples, and simple crafting tools. The two-dimensional felt banners that used to hang in the Christian churches of my childhood, bright blue and green pastoral scenes of birds, butterflies, and a crucifix inspired me. I would create something smaller, in a series of three, to capture the rise and fall of a pain episode.



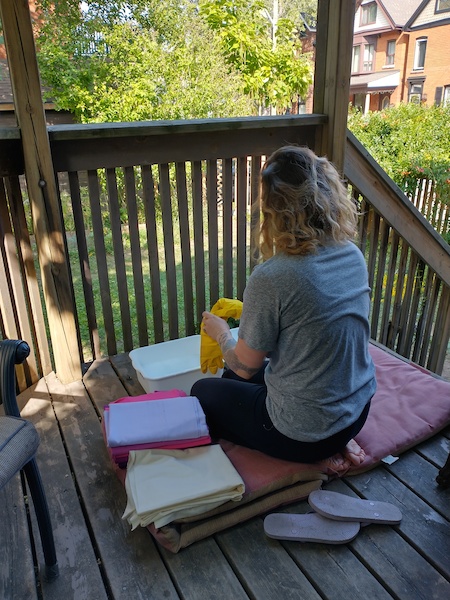
Once my health improved a couple of days later, I returned to my academic work and put the project on pause. But when alerted by signs of an approaching pain cycle, I drove across town to the Fabricland. I moved between racks of fabrics, touching each bolt until I found the corner containing a shelf of soft flannel. The immediate feeling of being soothed by the bright and pastel colored fabric demonstrated the “different perceptual systems” at play when encountering texture. [85] That weekend, I took the bag of fabric to a friend’s porch. I set up two buckets, with a cushion for my knees, and set to work, hand washing and rinsing each piece (Fig. 4). With moderate pain, fatigue, and nausea, I took the preparation process slowly. I took breaks between washing and rinsing each piece of flannel, standing to stretch and drinking water. After an hour and a half, I hung the pieces on the clothesline to dry in the breeze (Fig. 5).

A few days later in my bedroom, I experimented with cutting shapes and backgrounds. As I scheduled this activity for when I was sick and fatigued — when ordinary work was impossible — I limited each sitting to a maximum of two hours, again propped on a cushion on the floor with the materials spread around me. I found that the scissors I had purchased were too big; they were awkwardly heavy and strained my hand. The flannel wrinkled easily, and picked up lint from the floor. I realized I would never complete these images if they were hand sewn, so I opted for the crudeness of fabric glue instead. Over three months, I created this triptych. The simplicity of each image, both in their process and in the final result, is reflective of the hold sickness takes as it reorients your life. Pained, persistent, yet somehow spectacular, if only in the mediated moment of making meaning from within illness.
Evoking non-normative femininity and embodiment, this series is a gesture towards a sick and queer feminist reimagining of menstrual art informed by a disability aesthetic. My first piece, Flare, represents the eruption of pain (Fig. 1). This piece has a distinct horizon, directed towards a burgundy circle in the middle. The center of the piece is where the eruption emerges from, as overlapping magenta and purple snake-like shapes spread out towards the edges. Two blue eyelets are obscured by pink streaks. The piece has a sense of outward momentum and of expansion: the trajectory of a pain flare. The second piece in the series, Flood, moves the viewer’s gaze from left to right, as the image appears to propel across the background (Fig. 2). Amorphous purple and pink shapes struggle and compete against one another for dominance, bubbling across the surface. Flood symbolizes a take-over of the bodily organs as pain routes through them. Float, the final piece in the series, represents the body being invaded by trauma, illness, and medical intervention (Fig. 3). The organic shapes of deep purples and magentas are heavy against the lilac background, where the body lays unmoored. In a state of invasion — by cells, pain, and outside touch — the response of the self is to float. Taken together, these images form a visual narrative of negotiating a gendered chronic illness.
6_Conclusion
Beginning from my own experience in struggling for an endometriosis diagnosis, this article has argued that the conventional medical narrative of endometriosis is limited by normative views of female-assigned reproduction and fertility. Instead, a feminist disability studies lens provides the language to name endometriosis and endometriosis-like symptoms as a disabling chronic illness with myriad socio-economic effects. Analyzing endometriosis through a feminist disability justice framework privileges an intersectional understanding of illness, resisting the medical gaze and valuing non-normative embodiment. This opens up space to think about inhabiting the body in ways that do not prioritize ‘getting better.’ Healing, on the other hand, is a process without a beginning or an end, a state that is in constant flux. Feminist disability politics make room for healing as an embodied process untethered to outcomes. [86]
Art is one mode whereby disability politics can be articulated and circulated; a disability aesthetic grants inherent meaning to art produced at the axis of disability. Turning to an art-based practice has enabled me to articulate aspects of my chronic illnesses and embodiment that eschew language. A touch-based practice of expression gives meaning to color, shape, and texture. In the slow, methodical process of creating Flare, Flood, and Float, a cycle of pain is registered, narrated, and moved through. This article documents my efforts to reflexively theorize my own embodiment to articulate the affective quality of chronic illness through weaving together medical, academic, and arts-based conversations. Realistically, I may never receive a diagnosis of endometriosis; but in the event that I do, my chances for treatment and an enhanced quality of life improve. Either way, I will still seek a language to express my experiences, using poetry, prose — and perhaps a visual arts-based practice. Illness does not define my life as much as it colors it. Sensitive to the light, whorls of pink and purple, pushing through a cloudy fog.
_How to Cite
McKenna, Emma. “Material Shifts: Theorizing Endometriosis, Embodiment, and Experimental Art.” On_Culture: The Open Journal for the Study of Culture 11 (2021). <http://geb.uni-giessen.de/geb/volltexte/2021/16170/>.
_Endnotes
- [1] Thank you to Vanessa Lecavalier for her research assistance on menstrual art.
- [2] Emma M., “Endometriosis, or Modern Hysteria?” in GUTS Magazine, (March 31, 2016), n.p. accessed May 25, 2021, <http://gutsmagazine.ca/endometriosis-modern-hysteria/>.
- [3] Autotheory describes writing that combines autobiography with philosophy and theory. See Robyn Weigman, “Autotheory Theory,” in Arizona Quarterly: A Journal of American Literature, Culture, and Theory 76.1 (2020), 1–14; Lauren Fournier, Autotheory as Feminist Practice in Art, Writing, and Criticism (Cambridge: MIT Press, 2021).
- [4] Eve Kosofsky Sedgwick, Touching Feeling: Affect, Pedagogy, Performativity (Durham: Duke University Press, 2004), 3.
- [5] Sally Thorne, Janice McCormick, and Elaine Carty, “Deconstructing the Gender Neutrality of Chronic Illness and Disability,” in Health Care for Women International 18.1 (1997), 1–16, here: 6.
- [6] Andrew Horne and Carol Pearson, Endometriosis: The Experts’ Guide to Treat, Manage, and Live Well with Your Symptoms (London: Vermillion, 2018), 2.
- [7] Horne and Pearson, Endometriosis: The Experts’ Guide, 2–3.
- [8] Maya Dusenberry, Doing Harm: The Truth About How Bad Medicine and Lazy Science Leaves Women Dismissed, Misdiagnosed (New York: Harper One, 2018), 219.
- [9] Chris Bobel et al., eds., The Palgrave Handbook of Critical Menstruation Studies (New York: Palgrave Macmillan, 2020).
- [10] Horne and Pearson, Endometriosis: The Experts’ Guide, 7.
- [11] Kate Young, Jane Fischer, and Maggie Kirkman, “‘Do Mad People Get Endo or Does Endo Make You Mad?’: Clinicians’ Discursive Constructions of Medicine and Women with Endometriosis,” in Feminism & Psychology 29.3 (2019), 337–356.
- [12] Abby Norman, Ask Me About My Uterus: A Quest to Make Doctor’s Believe in Women’s Pain (New York: Bold Type Books, 2018), 46.
- [13] Dusenberry, Doing Harm, 222–225. Dusenberry explains how, beginning in the 1940s, doctors formed an association between incidences of endometriosis and women delaying the age of childbearing. By the 1960s, the label “the career women’s disease” emerged to explain why postponing or avoiding pregnancy caused endometriosis. In this theory, white women’s bodies became disordered as a consequence of selfishness. In contrast to white women, racialized women’s reports of menstrual pain were overwhelmingly dismissed or mis-diagnosed as Pelvic Inflammatory Disease; until the late 1980s, black and racialized women were not diagnosed with endometriosis.
- [14] Kate Seear, The Making of a Modern Epidemic: Endometriosis, Gender, and Politics (Abingdon: Routledge, 2014); See also, Maisha Johnson, “I’m Black. I Have Endometriosis—and Here’s Why My Race Matters,” in Healthline (2019), n.p. accessed September 8, 2020, <https://www.healthline.com/health/endometriosis/endo-race-matters>; See also, Emily Lipstein, “Treating Endometriosis as a Women’s Disease Hurts People of All Genders,” in Vice (November 11, 2020), n.p. accessed December 22, 2020, <https://www.vice.com/en/article/xgzxkk/treating-endometriosis-as-a-womens-disease-hurts-patients-of-all-genders>.
- [15] Virginia Kallianes, “Disabled Women and Reproductive Rights,” in Disability & Society 12.2 (1997): 203–222; Leonardo Pegoraro, “Second-Rate Victims: The Forced Sterilization of Indigenous Peoples in the US and Canada,” in Settler Colonial Studies 5.2 (2015), 161–73; Helen Rodriguez-Trias, “Sterilization Abuse,” in Women & Health 3.3 (1978), 10–15.
- [16] Horne and Pearson, Endometriosis: The Experts’ Guide, 143–146.
- [17] Dusenberry, Doing Harm, 224; Norman, Ask Me About My Uterus, 49.
- [18] Center for Endometriosis Care, “About Endometriosis,” in Centre for Endometriosis Care (1990, updated 2020), n.p. accessed September 8, 2020, <https://centerforendo.com/endometriosis-understanding-a-complex-disease>.
- [19] Fabi Jabr and Venk Mani, “An Unusual Case of Abdominal Pain in a Male Patient: Endometriosis,” in Avicenna Journal of Medicine 4.4 (2014), 91–94; Mark Shuster and Dhanya A. Mackeen, “Fetal Endometriosis: A Case Report,” in Fertility and Sterility 103.1 (2015), 160–62.
- [20] Elaine Denny, “‘I Never Know from One Day to Another How I Will Feel’: Pain and Uncertainty in Women with Endometriosis,” in Qualitative Health Research 19.7 (2009), 985–995.
- [21] Norman, Ask Me About My Uterus, 50.
- [22] The Endometriosis Network Canada. “About Us,” in Endometriosis Network Canada (2012, updated 2021), n.p. accessed May 25, 2021, <https://endometriosisnetwork.com/our-story>.
- [23] EndoAct Canada. “Introduction.” In EndoAct Canada (updated 2021), n.p. accessed May 25, 2021, <https://endoact.ca/>.
- [24] Pain Canada. “We Need Action to #Prioritize Pain,” in Pain Canada (updated 2021), n.p. accessed May 25, 2021, <https://www.paincanada.ca/>.
- [25] Mia Mingus, “Disability Justice is Simply Another Term for Love,” in Leaving Evidence (November 3, 2018), n.p. accessed May 25, 2021, <https://leavingevidence.wordpress.com/2018/11/03/disability-justice-is-simply-another-term-for-love/>.
- [26] Other key contributions to this development include: Michelle Fine and Adrienne Asch, eds., Women with Disabilities: Essays in Psychology, Culture and Politics (Philadelphia: Temple University Press, 1988); Rosemarie Garland-Thompson, “Feminist Disability Studies,” in Signs: Journal of Women in Culture and Society 30.2 (2005), 1557–87; Rosemarie Garland-Thompson, “Disability Studies: A Field Emerged,” in American Quarterly 65.4 (2013), 915–26.
- [27] Susan Wendell, “Toward a Feminist Theory of Disability,” in Hypatia: A Journal of Feminist Philosophy 4.2 (1989), 104–124, here: 105.
- [28] See further the following editorials: Rosemarie Garland-Thompson, “Integrating Disability, Transforming Feminist Theory,” in NWSA JournalSpecial Issue: Feminist Disability Studies, 14.3 (Autumn 2002), 1–32; Kim Q. Hall, “New Conversations in Feminist Disability Studies: Feminism, Philosophy, and Borders,” in Hypatia: A Journal of Feminist Philosophy Special Issue: New Conversations in Feminist Disability Studies, 30.1 (Winter 2015), 1–12; Nancy A. Naples, Laura Mauldin, Heather Dillaway, “Gender, Disability, and Intersectionality,” in Gender & Society Special Issue: Gender, Disability, and Intersectionality, 33.1 (Winter 2018), 5–18.
- [29] Cara E. Jones, “The Pain of Endo Existence: Toward a Feminist Disability Studies Reading of Endometriosis,” in Hypatia A Journal of Feminist Philosophy 31.3 (2016), 554–571.
- [30] Jones, “The Pain of Endo Existence,” 555.
- [31] Jones, “The Pain of Endo Existence,” 556.
- [32] Wendell, “Toward a Feminist Theory of Disability,” 110.
- [33] Horne and Pearson, Endometriosis: The Experts Guide, 190–191.
- [34] For other auto-theoretical narratives on gender, pain, and other chronic illnesses, see: Amy Berkowitz, Tender Points (Brooklyn: Nightboat Books, 2019 [2015]); Sonya Huber, Pain Woman Take Your Key, and Other Essays from a Nervous System (Lincoln & London: University of Nebraska Press, 2017); Porochista Khakpour, Sick: A Memoir (New York: Harper Perennial, 2018).
- [35] Lara Parker, Vagina Problems: Endometriosis, Painful Sex, and Other Taboo Topics (New York: St. Martins Griffin, 2020), 83.
- [36] Horne and Pearson, Endometriosis: The Experts’ Guide, 72–73; Norman, Ask Me About My Uterus, 47.
- [37] Kate Seear, “The Etiquette of Endometriosis: Stigmatisation, Menstrual Concealment and the Diagnostic Delay,” in Social Science & Medicine 69.8 (2009), 1220–1227.
- [38] Emma Cox, “Preface,” in Endometriosis: The Experts’ Guide to Treat, Manage, and Live Well with Your Symptoms, eds. Andrew Horne and Carol Pearson (London: Vermillion, 2018), ix–xi, here: ix.
- [39] Jones, “The Pain of Endo Existence,” 556.
- [40] Matthew Lionardi et al., “Deep Endometriosis: A Diagnostic Dilemma with Significant Surgical Consequences,” in Journal of Obstetric Gynecology Canada 40.9 (2018), 1198–1203; Centre for Endometriosis Care, “Excision of Endometriosis,” in Centre for Endometriosis Care (1990, updated 2020), n.p. accessed December 23, 2020, <https://centerforendo.com/lapex-laparoscopic-excision-of-endometriosis>.
- [41] On digital community and support groups, see: Horne and Pearson, Endometriosis: The Experts Guide, 182–183; Parker, Vagina Problems, 22–26; Norman, Ask Me About My Uterus, 206.
- [42] Sarah Maslen and Deborah Lupton, “Enacting Chronic Illness With and Through Digital Media: A Feminist New Materialist Approach,” in Information, Communication, and Society 23.11 (2020), 1640–1654. See further closed Facebook Groups, including Endometriosis Canada, and in the United Kingdom, Nancy’s Nook.
- [43] Jean A. Gilmour, Annette Huntington, and Helen V. Wilson, “The Impact of Endometriosis on Work and Social Participation,” in International Journal of Nursing Practice 14.6 (2008), 443–448.
- [44] Katherine C. Aquino and Joshua D. Bittinger, “The Self-(un)Identification of Disability in Higher Education,” in Journal of Postsecondary Education and Disability 32.1 (2019), 5–19.
- [45] Derrik Kranke et al., “College Student Disclosure of Non-Apparent Disabilities to Receive Classroom Accommodations,” in Journal of Postsecondary Education and Disability 26.1 (2013), 35–51.
- [46] Jennifer Marie Martin, “Stigma and Student Mental Health in Higher Education,” in Higher Education Research and Development 29.3 (2010), 259–274.
- [47] Karen Elizabeth Jung, “Chronic Illness and Educational Equity: The Politics of Visibility,” in NWSA JournalSpecial Issue: Feminist Disability Studies, 14.3 (Autumn 2002), 178–200.
- [48] Susan Wendell, “Unhealthy Disabled: Treating Chronic Illnesses as Disabilities,” in Hypatia: A Journal of Feminist Philosophy 16.4 (2001), 17–33, here 24.
- [49] Wendell, “Unhealthy Disabled,” 26.
- [50] Valorie A. Crooks, Michelle Owen, and Sharon-Dale Stone, “Chronic Illness and the Canadian Knowledge Worker: The Role of the Body and Embodiment in Shaping the Production of Academic Work,” in Working Bodies: Chronic Illness in the Canadian Workplace, eds. Sharon Dale Stone, Michelle K. Owen, and Valorie A. Crooks (Montreal-Kingston: McGill-Queens University Press, 2014), 196–209, here: 198.
- [51] Daniel Roy Torunczyk, “The PhD Employment Crisis is Systemic,” in Policy Options/Options Politiques (July 30, 2019), accessed December 13, 2020, <https://policyoptions.irpp.org/magazines/july-2019/the-phd-employment-crisis-is-systemic/>.
- [52] Jung, “Chronic Illness and Educational Equity,” 191.
- [53] Peiyun She and Gina A. Livermore, “Long Term Poverty and Disability Among Working-Age Adults,” in Journal of Disability Policy Studies 19.4 (2009), 244–256; David C. Stapleton, Bonnie L. O’Day, Gina A. Livermore, and Andrew J. Imparato, “Dismantling the Poverty Trap: Disability Policy for the Twenty-First Century,” in The Milbank Quarterly: A Journal of Population Health and Health Policy 84.4 (2006), 701–732.
- [54] DisAbled Women’s Network of Canada (DAWN), More than a Footnote: A Research Report on Women and Girls With Disabilities in Canada (February 2019), 1–194, here: 35, accessed December 12, 2020, <https://dawncanada.net/media/uploads/page_data/page-64/more_than_a_footnote_research_report.pdf>.
- [55] DAWN, More than a Footnote, 34.
- [56] Ernie Lightman et al. , “‘Not Disabled ‘Enough’: Episodic Disabilities and the Ontario Disability Support Program,” in Disability Studies Quarterly 29.3 (2009), n.p.
- [57] Valorie A. Crooks, “Income Assistance (the ODSP) and Disabled Women in Ontario, Canada: Limited Program Information, Restrictive Incomes and the Impacts Upon Socio-Spatial Life,” in Disability Studies Quarterly 24.3 (2004), n.p.
- [58] Council of Canadians with Disabilities, As a Matter of Fact: Poverty and Disability in Canada (2013), n.p. accessed December 13, 2020, <http://www.ccdonline.ca/en/socialpolicy/poverty-citizenship/demographic-profile/poverty-disability-canada>.
- [59] I have also been informed by the activist discourse of disability justice. See: Leah Lakshmi Piepzna-Samarasinha, Care Work: Dreaming Disability Justice (Vancouver: Arsenal Pulp Press, 2020).
- [60] Sedgwick, Touching Feeling, 14.
- [61] Johanna Hedva, “Sick Woman Theory,” in Mask Magazine (January 19, 2016), n.p. accessed May 19, 2021, <http://www.maskmagazine.com/not-again/struggle/sick-woman-theory>.
- [62] Luanne Martineau, “Not an Outsider Artist: An Appreciation of Judith Scott,” in Canadian Art (October 13, 2016), n.p. accessed December 4, 2020, <https://canadianart.ca/features/judith-scott-luanne-martineau>.
- [63] Amelia Rachel Hokule’a Borofsky, “Where Great Art Transcends Disability,” in The Atlantic, (December 13, 2012), n.p. accessed December 4, 2020, <https://www.theatlantic.com/health/archive/2012/12/where-great-art-transcends-disability/266184/>.
- [64] Martineau, “Not an Outsider Artist,” n.p.
- [65] Tobin Siebers, “Disability Aesthetics,” JCRT 7.2 (2006), 63–73.
- [66] Siebers, “Disability Aesthetics,” 63.
- [67] Siebers, “Disability Aesthetics,” 71.
- [68] Theresa Van Lith, “Art Making as a Mental Health Recovery Tool for Change and Coping,” in Art Therapy, 32.1 (2015), 5–12; Judith Pizarro MA (2004) “The Efficacy of Art and Writing Therapy: Increasing Positive Mental Health Outcomes and Participant Retention After Exposure to Traumatic Experience,” Art Therapy, 21.1 (2004), 5–12.
- [69] Patricia Leavy, Method Meets Art, Third Edition: Arts Based Research Practice (New York: Guilford Press, 2020), 16.
- [70] Leavy, Method Meets Art, 11.
- [71] Susan Finley, “Arts Based Research,” in Handbook of the Arts in Qualitative Research: Perspectives, Methodologies, Examples, and Issues, eds. J. Gary Knowles and Ardra L. Cole (Thousand Oaks, CA: Sage Publications, 2008), 71–82.
- [72] Lekkie Hopkins, “Women’s Studies and Arts-Informed Research: Some Australian Examples,” in Handbook of the Arts in Qualitative Research: Perspectives, Methodologies, Examples, and Issues, eds. J. Gary Knowles and Ardra L. Cole (Thousand Oaks, CA: Sage Publications, 2008), 557–567, here: 567.
- [73] Catherine G. Kelly, Shirley Cudney, and Clarann Weinert, “Use of Creative Arts as a Complementary Therapy by Rural Women Coping With Chronic Illness,” in Journal of Holistic Nursing 30.1 (March 2012), 48–54; Frances Reynolds and Sarah Prior, “‘A lifestyle coat-hanger’: A Phenomenological Study of the Meanings of Artwork for Women Coping with Chronic Illness and Disability,” in Disability and Rehabilitation 25.14 (2003), 785–794.
- [74] Frances Reynolds, “Conversations About Creativity and Chronic Illness: Textile Artists Coping With Long-Term Health Problems Reflect on the Origins of Their Interest in Art,” in Creativity Research Journal 15.4 (2003), 393–407; Frances Reynolds, “Reclaiming a Positive Identity in Chronic Illness through Artistic Occupation,” in OTJR: Occupation, Participation and Health 23.3 (July 2003), 118–27.
- [75] Ora Prilleltensky, “Women with Disabilities and Feminist Therapy,” in Women and Therapy 18.1 (1996), 87–97.
- [76] Chun-shan (Sandie) Yi and Catherine Hyland Moon, “Art Therapy and Disability Studies,” in Art Therapy, 37.2 (2020), 59–61.
- [77] Solomon (Ellie) Kammer, “solomonkammer.com”, accessed December 23, 2020, <http://solomonkammer.com/>.
- [78] Emily Blatchford, “Ellie Kammer: The Artist Making Art of Endometriosis,” in The Huffington Post (March 10, 2017), n.p. accessed December 23, 2020, <https://www.huffingtonpost.com.au/2017/10/02/ellie-kammer-the-artist-making-art-of-endometriosis_a_23230417/>.
- [79] Chris Bobel and Breanne Fahs, “From Bloodless Respectability to Radical Menstrual Embodiment: Shifting Menstrual Politics from Private to Public,” in Signs: Journal of Women in Culture and Society 45.4 (2020), 955–983.
- [80] Jennifer Nelson, “Historicizing Body Knowledge: Women’s Liberation, Self-Help, and Menstrual Representation in the 1970s,” in Frontiers 40.1 (2019), 39–61; Camilla M. Røstvik, “Blood Works: Judy Chicago and Menstrual Art since 1970,” in Oxford Art Journal 42.3 (2019), 335–353.
- [81] Ruth Green-Cole, “Gendered Heterotopias: Creating Space for Menstrual Blood in Contemporary Art,” in Landscapes of Monstrosity, eds. László Munteán and Hans Christian Post (Leiden: Brill, 2016), 39–47.
- [82] Daniela Tonelli Manica and Clarice Rios, “(In)Visible Blood: Menstrual Performances and Body Art,” in Vibrant: Virtual Brazilian Anthropology 14.1 (2017), n.p; Chella Quint, “From Embodied Shame to Reclaiming the Stain: Reflections on a Career in Menstrual Activism,” in The Sociological Review 67.4 (2019), 927–942.
- [83] Bee Hughes, “Challenging Menstrual Norms in Online Medical Advice: Deconstructing Stigma through Entangled Art Practice,” in Feminist Encounters: A Journal of Critical Studies in Culture and Politics 2.2 (2018), 1–15. Note that Hughes uses poetry and visual art to critique the normative discourse of menstruation.
- [84] Sedgwick, Touching Feeling, 17.
- [85] Sedgwick, Touching Feeling, 15.
- [86] adrienne maree brown, “Healthcare vs. Healing,” in adrienne maree brown, (February 20, 2011), n.p. accessed May 25, 2021, <http://adriennemareebrown.net/2011/02/20/healthcare-vs-healing/>.