Pot and Power
The Role of the Nonhuman in a Very Human Business



1_Introduction: Relating Pot to Power
The significance of material objects (which we define as the ‘nonhuman’ in this paper) in the formation of culture and cultures is unchallenged, not just since the term “material turn” was coined some decades ago. [1], [2] In our following deliberations, we explore the constitutive role of the nonhuman in historical and contemporary socio-cultural formations in a context which is said to be ‘human-centered’: the daily care of people of various ages with disabilities or illnesses. Accordingly, we define material objects which are produced for and/or used in care and nursing settings (such as toilet chairs, urinals or incontinence draw sheets) as the non-human: they are the consumable material appliances utilized when people care for other people.
The formation of practices, politics, and the distribution of knowledge within care and nursing has always been deeply intertwined with the very formation of culture and cultures. This is particularly apparent when focusing on issues of cleanliness in nursing and care, which are considered to be civilized and cultivated, and includes the way we deal with excrement. [3] Supporting bodies during excretion is a central part of nursing and care work in almost every culture. [4] We will show that material objects play an important role not only in dealing with carers’ tasks, but also in enabling people to deal with excrement and excretion in a culturally appropriate manner. Alongside ‘correct’ behavior in care and nursing practices we find that when it comes to supported excretion, the ‘correct’ use of material objects is of equal importance when nurses and care givers have to organize the space for, and the situation of, excretion for people who are unable to do this alone in appropriate and suitable ways.
This is a situation where the pot is closely related to questions of power: as we will elaborate, certain practices of care and nursing involve special situations — supported excretion, for example — which may be fraught with shame, which involve touching and being touched in the genital area and in which one has to expose oneself to other people’s feces or expose one’s feces to another person. Here we understand power as a restrictive and enabling force, in the sense of Michel Foucault’s concept of ‘biopower,’ albeit on a microlevel, enacted in interactions between people and material objects. [5] By analyzing the role that material objects play in care and nursing interactions, we open up a multiplicity of aspects: from the concrete objects (that is, toilet chairs or urinals) and their materiality, the contexts in which they are applied (that is, nursing and care for ill or older people), to collective normative ideas about feces (or dirt) and the bodies excreting them or how supportive excretion should be managed (professionally) in care and nursing settings (how to touch the person being helped with excretion, how to deal with shame and so on).
In social and cultural anthropology, human excretion is a subject which has, as yet, been paid little attention: [6]
The anthropological treatment of the toilet and — to be more precise — human defecation reflects that cultural taboo. Toilets and defecation practices do not appear on the pages of ethnographic accounts. Mary Douglas’s famous dictum that ‘dirt is a matter out of place’ also proves its right in anthropological handicraft. Consciously or not, anthropologists almost universally avoid the topic. [7]
This is despite the fact that the anthropologist Joseph B. Loudon called for research into defecation as long ago as 1975: “Like sex and food, feces and defecation have a social component as well as a biological one […] deciphering them is relevant to the study of small-scale social relations, of concepts of intimacy, privacy and distance, of the link between thinking and stinking.” [8]
Research into the history of care has not examined the topic yet, either. The few works from German-speaking countries to have engaged with carers’ specific tasks have omitted the topic of how people deal with supported excretion and feces. The only exception to this is Astrid Stölzle’s work on the care of sick soldiers in the First World War, [9] which investigates how infectious excretions are actually dealt with in the context of epidemiological care and describes various measures taken to counter different degrees of sickness. [10] In the history of medicine, while the subject of excrement is addressed in the context of the four humors as part of a scientific concept (see below), there is no focus on the behavioral aspects of dealing with it. In the context of research into the history of care and nursing, especially, there has as yet been no confrontation with the multifaceted aspects of supported excretion, excrement and defecation.
Based on empirical research into historical and contemporary institutional settings of care (derived from material culture studies, object-centered historical analyses and multi-sited ethnography), we analyze the complex intermingling of humans and artifacts in the endeavor of supported excretion. It is our theory that material objects are used to bring about order where there is disorder caused by human waste. At different times, different notions about care or how to deal with bodily dirtiness are also reproduced. As we will show, the material culture of care in this context points to ways in which being human (physically, mentally, and emotionally) is fundamentally affected by the nonhuman, in our case by those material objects which support excretions for dependent persons. They play a central role in negotiating power in delicate nursing situations, in producing social control over ‘dirty’ bodies which are cared for.
In the second part of this paper we will offer a brief overview of how the question of nursing, dirty bodies, and dirty work has been explored in historical, anthropological, and sociological research. As we will demonstrate, this rather taboo topic has not yet been analyzed with regard to the role played by ‘nonhuman actors’ or material objects in solving the issue of handling dirty bodies. This desideratum will be addressed in the third section, in which we present the main findings of our own research on the role material objects had and have in supported excretion. In the final part, we present our main findings on how material objects help in the negotiation of ‘discreet’ and ‘good’ nursing care when it comes to excretion, or how complexly intertwined the relationship between ‘pot and power’ is.
2_Nursing as Dirty Body Work? The Cultural Orderings of Dirt, Bodies, and Nursing
The Cultural Effects of Dirt
According to Mary Douglas, creating social order is a central characteristic of culture. In that respect, dealing with dirt is one of the central classification schemes used to create social order and draw the lines between good and bad, right and wrong, inside or outside a ‘civilized’ community: “Dirt offends against order. Eliminating it is not a negative movement, but a positive effort to organize the environment.” [11] Douglas points out that a society’s definition of what is dirty is socially constructed and depends greatly on context. Sjaak van der Geest [12] follows Douglas’s argument, postulating that “[e]xcretions of the body are the most strongly felt matters out of place and, therefore, the most informative pointers of cultural boundaries and identity construction.” [13] Distinguishing between what is clean and what is dirty is one of the basic differentiations applied in the socialization of people in their culture: “Children are taught not to touch what comes out of their body, because it is ‘dirty.’ […] Defecation — like health and illness, and the senses — seems an eminent subject to study the complex intertwinement of what we call ‘nature’ and ‘culture’.” [14]
In what are known as Western societies, some basic, normative notions have evolved since the dawn of the modern bourgeois era according to which feces are a private matter; a truly solitary affair. [15] The subject is banned from the public sphere and considered strictly off limits: it is not seen or talked about. [16] This has not always been the case, but is something which has transpired throughout history. In other words, just as culture cannot be seen as something static or clearly delimited, when it comes to feces, the boundaries of what is culturally appropriate are subject to constant change.
Thus, for example, the modern taboo contrasts with the understanding in the ancient world, where excrement and defecation did not lead to such major disruptions of the social order as they do today. They were not as strictly banned from the public sphere or seen as a purely private matter; something which can be observed from the public latrines in ancient Roman cities, where people sat on the lavatory together in what was, therefore, not the ‘smallest room’ but in fact a big room (or even a building). They were, in fact, public places where people gathered not only to use the bathrooms, but also to meet and chat with neighbors, business partners and so on. [17] Until medicine developed into a discipline based on the natural sciences during the 19th century, the concept which guided our understanding of the body in terms of health and illness was that of humoralism (the four cardinal humors), which ascribed a specific role to feces. To maintain human bodily health, it was claimed that the proportions of the bodily fluids (humors) of blood, phlegm, yellow bile and black bile needed to be in balance. According to this view, excrement was used to excrete all harmful substances which the body ingested but could not ‘assimilate’ into its nature and which could thus impinge upon the humors. [18] The stench was considered a measure of the quantity of filth and dirt ingested and now excreted. [19] During the 19th century, communication about urine, feces, and their manifestation in the form of belching, flatulence and so on, was banned from the public sphere, and has since counted among the private bodily activities carried out by individuals alone, behind closed doors. [20] In public, those doors have continued to be strictly divided according to a binary logic of two genders. [21] If it was not possible for the excretion to take place in a specially designed room of the kind which soon entered tenements (shared lavatories on landings) and later apartments, the furniture required, such as commodes, was designed (unlike in ancient times) so that it did not immediately reveal its purpose.

The way we deal with and interpret dirt provides clues about the moral concepts within our culture. One key example of the amount of information which can be provided is the extent to which this affects even the smallest social fields or units. Within every field of work, specific standards of order and disorder are set down for each profession with regard to dirt (which, apart from anything else, offers ways of distinguishing one occupational field from another). This is especially evident with regard to care-related occupations: [22] dealing with or touching excrement produced by people who are not, for example, one’s relatives, tends to find more acceptance in care than in other occupations, among bank workers, for instance. [23] In the following, we will show that the cultural status of dealing with dirt, in this case with excrement and the process of defecation, proves not only to be socially constructed and dependent on context. In fact, this has far-reaching effects on a profession’s reputation, and is one of the reasons why care-related occupations have been, and still are, seen as dirty.
Nursing as Dirty Body Work
In the wake of the change in the modern bourgeois era described above, during which excretion came to be seen as an individual’s own responsibility and was increasingly relegated to the realm of privacy, [24] this became a problem for all those who could not or could no longer organize their own excretions and required assistance with their bowel movements. As excretion and excrement have been conferred the status of dirt, in the sense of Douglas’s concept of social order, this social order is disturbed by all those people who can no longer cope with the situation alone, and therefore cannot resolve it adequately for society. With the advent of bourgeois society, bodies, their orifices, and their excretions thus increasingly became a source of ambivalence, and the body came to be seen “as a site of social control.” [25]
The sociologist Erving Goffman took this interpretation even further, seeing the (human) body as a central medium for creating a bourgeois identity: people use their bodies to express different personal aspects in different situations, thus demonstrating or portraying their membership in a community or society. To turn this argument on its head, this means that in every (social) situation there are characteristic normative expectations regarding people’s posture, appearance or bodily regulation. If these expectations are not met, or if people deviate from them, this leads to feelings of embarrassment or shame. [26] Such emotions are a particularly strong indication that these are no longer ‘normal’ social situations; the limits of what is just about acceptable as the social order, as ‘normality,’ have been reached.
This is precisely the kind of situation in which people in need of care are placed when they are not capable of going to the toilet alone because of illness, ageing or disability. They experience an ‘abnormal’ case of organizing excretion, as they cannot manage it unassisted. Here, it is the carers’ task not only to enable them to relieve themselves, but also to help them do so in a manner complying as closely as possible with cultural standards in each situation. Thus Dreßke, among others, notes that “severely ill patients are now afflicted with the stigma of a failing body in a particularly extreme manner, relating not only to the illness itself but, especially to its side effects, which the care work is then based upon. Carers are principally entrusted with the task of ensuring the body functions at its physical limits.” [27] It is this involvement with intimate, ‘disgusting’ bodily functions such as defecation, and the general cultural status of dirt, as described above, which confers the label ‘dirty work’ on care work. Moreover, this has fundamental effects on the status of carers: “dirt (that is, human excrement) is so powerful that the position of people who deal with it equals the position of dirt in a society.” [28] The standing of a job or occupation is thus influenced by the generally dominant means within a society of differentiating people based on dirt: “In these ways we begin to conceive of the importance of dirt and dirty work in terms of characteristics that define, divide and stigmatize — dividing practices separating in-groups (clean-us) from out-groups (dirty-them).” [29] This directly affects nursing.
In nursing, the focus is on bodies to a particularly great extent. Bodies are touched in a manner which reflects power, and ‘normal’ bodily distances of the kind which preserve people’s intimate spheres outside hospitals or care homes are not maintained. [30] For this reason, the manner in which the patient’s body is treated, a central element of nursing, has a major effect on the social order within the care setting: “One of the notable aspects of most health care is its overt interest in the body. Healthcare workers — whether doctors, nurses, students or healthcare assistants — work with people’s bodies on a daily basis, frequently through the medium of touch.” [31] This sometimes powerful “professional touch” can be understood as “an outward manifestation of power and authority, with the powerful having a seeming right to touch the relatively powerless.” [32]
The touches involved in nursing and care are, however, also seen as sensitive and feminine, which means they appear pleasant, rather than threatening or powerful.
Thus nurses who do ‘body work’ involving touching are seen to be of lower status (Van Dongen and Elema, 2001) […]. In this respect, nursing work, women’s work and dirty work can be seen to be inextricably linked (Bolton, 2005) through association with the intimate care of bodies (culturally defined feminine) and with the private realm, where much of women’s work and ‘care’ takes place (Bolton, 2005). [33]
In this ambivalent situation, nursing is seen as a special form of “body work.” [34]
In this setting, nursing is thus constructed as ‘dirty body work.’ Both the way that people deal with dirt, and the view that nursing, as a truly feminine task, is seen as ‘simple’ work on and with the human body, are reasons why care professions continue to receive so little recognition within society. [35]
In view of the attributes ascribed to nursing work and its symbolically charged nature as dirty body work, this poses the question of how cultural notions of dirt and dirty bodies are and have been addressed within nursing. In which ‘culturally fitting’ ways have the challenges related to this delicate business been resolved? As we will show in the following section, material objects have played a central role historically and continue to do so today.
3_Material Culture of Care and the Duty of ‘Dirty Work’
Research Design
The focus of our work is on the non-human, understood as material objects that are and have been produced for and/or used in modern and historical care settings, which are involved in care work that entails the interactions of people and material objects. We conceive this interaction as being influenced by the socio-cultural contexts they are embedded in — among others, the hegemonic, normative ideas about care and nursing. However, with regard to the specific case in question, that of supported excretion, material objects actually make care possible in the first place.
Unlike the research work on dirty work and body work referred to in Chapter 2, we assume that care is influenced to a significant extent by material circumstances, by “non-human actors.” [36] For this reason we take an object-related approach in our research: when analyzing arrangements and situations within care, the starting point of our investigations are always the concrete objects in use.
By researching supported excretion, we are focusing on an area which has not only been the subject of scarcely any research, but which also offers a particularly wide range of potential explanations for culture and the cultural ramifications of being human, as opposed to non-human. Or, as van der Geest puts it: “Body products — and feces in particular — seem very tangible metonyms of bodily presence in the world. They could be ‘key informants’ for understanding the meaning of body and embodiment in the context of culture.” [37]
There is now some research work investigating situations of supported excretion, [38] but the non-human or material aspect of care has been ignored. To date, insufficient attention has been paid to the historical and contemporary significance which material objects may have in this field. We address this by focusing on nursing and care settings in German-speaking areas. In the next section, we discuss nursing practices from a historical perspective, focusing on institutional nursing arrangements in the 19th and 20th centuries. Following this, we consider contemporary nursing practice in institutional care for the elderly using a case study of a nursing home in Germany.
Object, Behavior and Cleanliness: The Pot, Power, and Dirty Nursing Work from a Historical Perspective
From a historical point of view, the first part of this investigation focuses on the practice of nursing in the 19th and early 20th centuries. Work on this subject arises from the sub-project on historical objects used in nursing, part of the joint project “Care and Things” [39] researching the material legacies of care preserved in collections covering this topic. As the situation is more than poor for that period in terms of sources from the carers’ perspective, examining objects and following their traces in normative literature offers an opportunity to shed light on fields of practice. Comparing subsequent editions of the most widespread German-language nursing textbook (from the Charité hospital, Berlin) and textbooks published by other doctors in Berlin, reviewing them purely in the context of how objects were used reveals the manual techniques, methods, and behaviors which developed and became established over a period of many years. This object-centered analysis can be used to uncover the strategies adopted by care practitioners dealing with defecation, micturition, and excrement. Analyzing the range of items supplied by the manufacturers of nursing equipment over time also shows the variety of material solutions provided to ensure that supported excretion could take place both in and out of the bed. In this study, strict attention is paid to the question of how people deal with dirt and dirty bodies.
How did professionals deal with the excretion of feces and urine which, in the case of patients confined to their beds, could not take place in absolute privacy behind closed doors, as etiquette had recently begun to demand, but required the assistance of another person to provide care? Natural boundaries of embarrassment and intimacy were transgressed in these situations — was this subject addressed, and what was the role of objects and their handling? Here, the historical viewpoint appears interesting to the extent that nursing only began to develop as a regulated profession during the 19th century. This was the first time that borderline situations dealing with material objects which were ‘out of place,’ as defined by Mary Douglas, were being addressed in printed books explicitly written to train nursing staff. As normative sources, textbooks show what carers were required to know, offering an insight into how professionals should manage these taboo moments for the carers and patients, and what role objects played in this process.
Tracing the Pot
Unlike modern nursing textbooks, those from the 19th century were not divided into specific nursing topics and concepts as we know them today. Thus, they did not contain the topic of ‘excretion’ and its related objects, knowledge, and fields of practice. In 1832, a combination of the chapters “Characteristics of an orderly,” “On sheets,” and “On support with bowel movements and chamber pots” [40] paints an overall picture of the required nursing duties in this respect. Sixty years later, the use of bedpans and urinals and methods for dealing with excretion have migrated to the chapter on “Patient observation.” At the beginning of the 20th century, they are to be found in the sections on “The sick chamber in general,” “Cleanliness in nursing” and “Assistance for people with symptoms of disease.” All these sections refer to the variety of equipment with their attendant differences in design and materials and corresponding advantages and disadvantages. In 1807, we are informed of bedpans made of tin, sheet iron, and wood. [41] In 1832, a textbook by Johann Friedrich Dieffenbach mentions bedpans almost exclusively made of tin being used to dispose of fecal matter, whereas tin was supposed to be avoided in urinal pots and preference given to those made of porcelain. [42] Nursing staff were supposed to be aware that urine could form stinking crusts in the latter which, in turn, could lead to unpleasant smells and insalubrious vapors. Almost 100 years later, nurses were expected to know that warmed glass bottles were best for excreting urine in bed — bottles “which, for women, should usefully have an opening in the shape of a shell or boat.” [43] This list of information about materials went on to include, for example, the advantages and disadvantages of bedpans with cloth covers, the practicability of those made of rubber or the risks of those made of glass — however, these examples should suffice. It is clear that the objects are being used to convey professional information. [44]
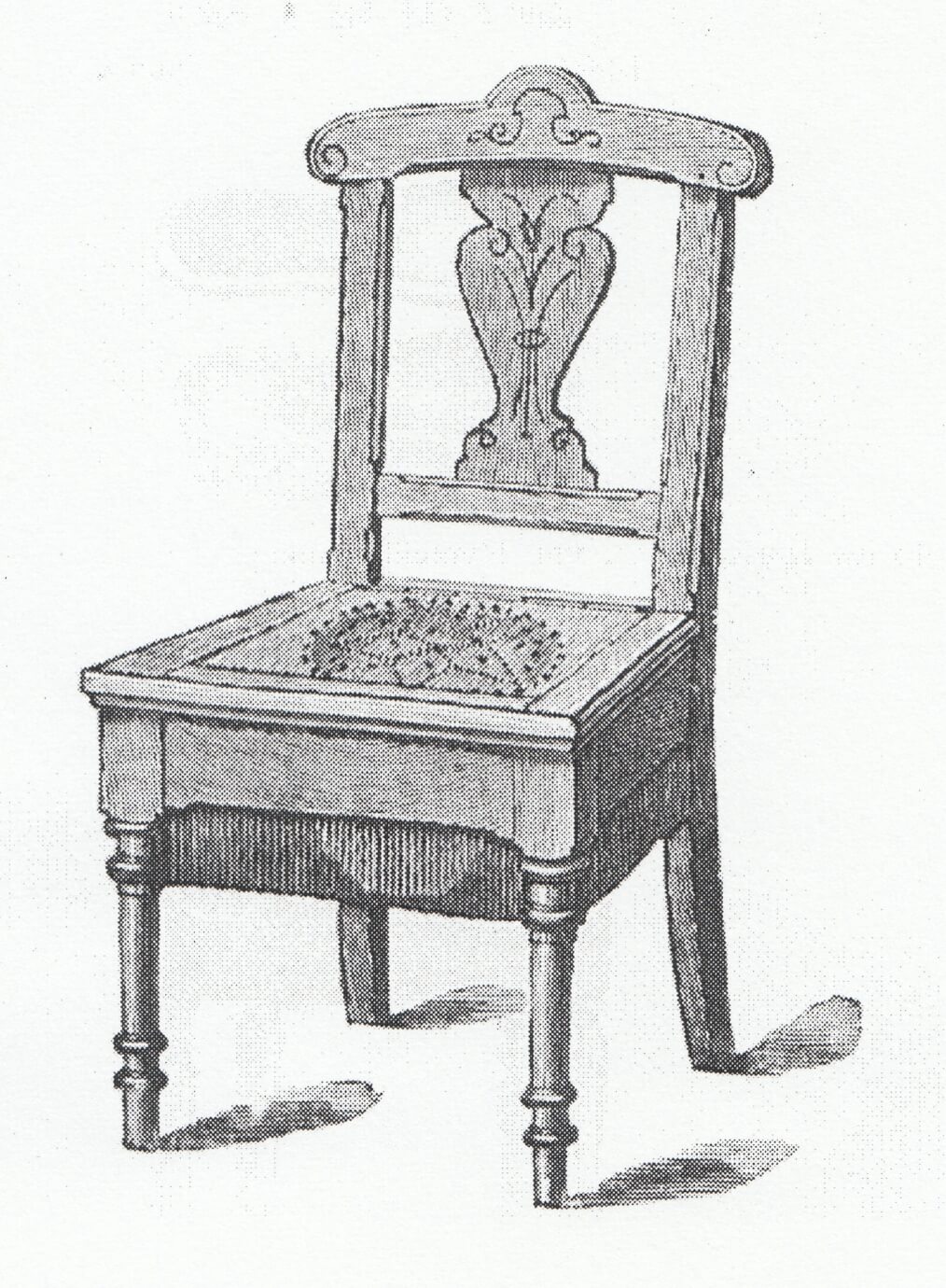
With this in mind, when one examines a catalogue of instruments from the turn of the 20th century, there seems to have been an incredibly wide range of designs for bedpans and urinals. At first sight, the variety of gender-related shapes shown in historical manufacturers’ catalogs is surprising. The male inventors, often doctors, and the producers of the items, who were also male, do seem to have had both sexes in mind. At the same time, however, textbooks also describe the use and materials of various gender-specific items, whether it was the simultaneous use of the bedpan and urinal by men, as early as 1832, [45] or a description of the shape of urinals for women, for example in 1896. [46] Close stools, necessary stools or night stools, [47] as the precursors of the modern toilet commode or chair were once known, were just as ‘ungendered’ as today, but there was a very wide range of furniture designs. The designs are, however, visibly discreet, as at first sight the chairs look like regular seats thanks to their decoration and appearance. One aspect contributing to this is the addition of a lift-up seat, not only making the chair multifunctional, but also making the bowl discreet (see illustrations above).
To care for and look after patients well, in the case of the inhibitive topic of excretion in particular, it is necessary either to acquire the best equipment or to use the equipment available correctly. Knowledge about material properties, design, and appropriate cleaning are essential prerequisites for this, as they are the only way to maintain a professional distance in the taboo circumstances of ‘dirty work.’
Dirty Work and Professional Interaction
In 1832, the physician and nursing book author Johann Friedrich Dieffenbach was fully aware of the fact that carers thus find themselves at the heart of ‘dirty work.’ Among the fundamental required characteristics of nurses, he wrote:
Orderlies may not exhibit disgust; they have to be able to see, smell and touch the most disgusting things, as it is their job to deal more with unpleasant and revolting things than with pleasant and agreeable ones. An orderly who wrinkles his nose when carrying out the patient’s stool is not doing himself any favors; he should, instead, examine the fecal matter well and remember what it looks like and how it smells; … the physician will ask him about it. The feces cannot, after all, always be preserved to show to the physician as it would pollute the chamber or the house, and it is generally enough for the orderly to provide a good description of it. [48]
Thus, while the patient and surroundings are to be kept away from feces as much as possible, the nurse is explicitly expected to expose him- or herself to excrement for the purpose of medical diagnosis, and by doing so in fact proves his or her medical competence.
Nurses also prove their professionalism by dealing with patients (and their excretions) fittingly, as shown by an excerpt from 1909: “Unappetizing work such as cleaning pots must never be carried out in the sick chamber; if this is unavoidable, it must be done out of sight of the patient if possible.” [49] This clearly shows how dealing properly with material objects ‘out of place’ is a sign of professional nursing.
From 1900 on, nurses were expected to demonstrate by their behavior that, in addition to knowing about issues related to cleanliness, they were also aware of those related to embarrassment. It was on the subject of using equipment in the bed that the subject was broached of transgressing the bounds of acceptability. The section on “Tasks carried out upon the patient’s body,” for example, reads: “When handling patients’ limbs it will always be necessary to lift the bedspreads; when handling their torso and entire body it may be incumbent upon the nurse to protect them against unpleasant chills which are often not without risk, and often to protect their modesty.” [50] Moreover, it is also important how patients are treated following the situation experienced as dirty:
Nurses are to perform the thorough hand wash which is always immediately necessary after such tasks (cleaning pots) in such a way that the patient sometimes notices, but without drawing particular attention to it. If possible, the nurse should seek to avoid touching the patient’s face or hands, or giving the patient food, shortly after tasks of this kind. [51]
The patient’s embarrassment and the nurse’s apparent lack of embarrassment in dealing with it also comes up at a later point, [52] the aim being to be as discreet as possible while also avoiding embarrassment. [53]
Regarding the period from the 19th to the early 20th century, it can be said that when it came to supported excretion, the main focus was on medical and hygienic aspects and how to deal with feces properly. Although from the beginning nurses’ codes of conduct on interacting with patients gave attention to the idea that nurses should not display disgust towards patients, and hence demonstrate their professionalism, patients’ embarrassment at their privacy being invaded is not explicitly addressed until the start of the 20th century. Nevertheless, from a historical perspective, it can be stated that specific knowledge of objects’ material properties resulted in a way of handling patients which served to manage necessary touching and so framed the nursing interaction as professional. This professional interaction should lead — along with the fulfillment of medical needs — to a satisfying and reassuring situation for the patient who was confronted with a shame-inducing and embarrassing situation whilst in need. The question of power relations, engendered by the dependence of the patient on the nurse, was answered by one of the central duties of nursing: the support of the patient’s well-being. The professionally-framed acts of dealing with dirt and intimate touch should lead to a suitable outcome for the patient.
The fact that, even today, supported excretion remains more complex than it might appear at first sight is demonstrated by the following description of modern ways of organizing supported excretion, using the example of the toilet chair.
Pot, Power, and Dirty Body Work: Contemporary Examples of Nursing Interactions with a Toilet Chair
In our investigation of contemporary nursing practice we focus on the province of institutional elderly care. In this field, in contrast to nursing for sick people, supported excretion is a far more pronounced element of everyday work due to the needs of elderly recipients of care. Due to demographic change, elderly care has become the fastest-growing field of nursing today. The reflections presented here on supported excretion in elderly care are based on a sub-project on the social order of things in nursing practice, which is also part of the joint research project on “Care and Things.” [54] An examination of the microlevel of nursing interactions between people and material objects, this sub-project studies the role that material objects can have in nursing practice and how they help (or hinder) the creation of the socially shared realities, self-evident truths and interpretational schemes [55] which influence the field of nursing. This inductive research project follows the approach of ethnomethodology and studies of work, mainly examining the question of how material objects are used to produce and reproduce not just social order in the form of powerful social relationships, but also notions of ‘normality’ (including those which influence normative discourses). A case example has been selected to investigate the effect which material objects have today, as part of everyday workflows in care settings. The aim is to look beyond specific, situational uses of material objects within interactions and to draw conclusions about everyday workflows, relationships, and moral concepts in the care institutions examined. To this end, instruction manuals and textbooks are also analyzed, and semi-structured narrative interviews carried out with nursing staff.
In the following, central results on dealing with excretions, reconstructed from the sub-project on the social order of things in nursing practice, are set out based on the example of the use of toilet chairs in elderly care. The toilet chair is suitable for investigation as a central item used in nursing for several reasons, one key reason being that it also offers an in-depth historical insight. Mainly known until the middle of the 20th century as a commode, close stool or night stool, the toilet chair has undergone a ‘career’ of use in nursing. As an exemplar, it can be used not only to trace back topics related to contemporary nursing settings, but also to follow their historical paths. This enables us to contrast the main findings of the research on contemporary practices with those reconstructed for the 19th and 20th centuries outlined in the previous section and, consequently, to open up an interdisciplinary dialogue. As the following descriptions show, the toilet chair today is used in nursing to fulfil discursively influential notions about carers’ professionalism or ‘good nursing’ — not least because those carers execute power over those they care for while handling the chamber pot or, in this case, the toilet chair.
Materiality of the Toilet Chair

Figures 3 and 4 show the toilet chair model which was to be found in almost every resident’s room in the nursing setting investigated, a nursing home for the elderly. In this nursing home the toilet chair was omnipresent and assigned a wide range of functions. Besides being used for excretion it was also used for personal care and hygiene or to transport residents for short distances. In the right-hand illustration above, the seat is folded down, giving the toilet chair a neutral appearance. In this position it is not immediately recognizable as an item used for excretion. Its shape (the seat and backrest) are reminiscent of a regular chair or, due to the rollers, a wheelchair. Above the backrest there is a handle indicating that the toilet chair can be pushed by another person apart from the person sitting on the chair. The brakes also seem designed to be operated by another person, as they are also fitted at the rear. The folding down seat also gives it a ‘discreet’ impression, as the opening for excretion can be covered up.
In terms of materials, the toilet chair mainly features subtle, restrained colors (black, gray and white) and tough materials. The frame is made of matte steel, the seat and backrest are made of PVC, the armrests are covered with thermoplastic material and the attachment for the toilet pot and the seat around it are made of synthetic polymer — all materials which are easy to wipe down and clean effectively. According to the operating instructions (which are not attached to the chair), it weighs around 14 kg and can bear a maximum weight of 160 kg. In contrast with its historical precursors (see Chapter 3 and Figs. 1 and 2), the toilet chair is made up of materials which, at the first appearance, provide the possibility for safe and hygienic usage while working discreetly.
Toilet Chairs in Situational Nursing Action and Interaction: A Case Example
In the nursing home, toilet chairs were observed to be employed and used in various ways: to transport residents, to hang towels on, to take showers and, last but not least, for excretion. The latter will now be described as a case example from an incident observed during ethnographic field work in one of the residential groups at the nursing home. The following is an excerpt from an observation protocol, in which the nurse (Mr. Kusic) helps one of the residents (Gustav) to use a toilet chair.
Mr. Kusic is on his way to the kitchen and meets Gustav in the hall, who tells him he needs to use the bathroom. He takes the carafe in his hand into the kitchen, then goes into Gustav’s room, where he pushes the wheelchair which Gustav is sitting in up to the bed. Gustav takes hold of the foot of the bed and stands up, with Nurse Kusic standing behind him and reaching under his arms. As Gustav stands there, Mr. Kusic pushes the wheelchair back and rolls the toilet chair behind the resident. The nurse helps Gustav to pull down his pants and underpants, and the resident sits down on the toilet chair. Mr. Kusic then puts a red string with an emergency button on the bed in front of Gustav and tells him to ring when he is ready.
[Not mentioned in the report: while Gustav sits on the toilet chair, Nurse Kusic visits two other residents and is away for about an hour.]
As Mr. Kusic is going along the hall towards the nurses’ room, he hears Gustav calling for him out of his room. He goes into the room, where Gustav is still sitting on the toilet chair. There is a slight smell of urine. Mr. Kusic asks me if I can get him some gloves out of the bathroom, and I do. He puts on the gloves and helps Gustav get up, holding onto the foot end of the bed, and pulls up his pants. He then pushes aside the toilet chair and pushes the wheelchair behind Gustav, who sits down on it. Mr. Kusic folds the foot rests up into place and sets the resident’s feet on them, asking ‘Why didn’t you ring?’ Gustav says something quietly [which I find hard to hear] and Mr. Kusic nods. Shortly after, he pushes Gustav out of his room, asking him if he would like something to eat.
The procedure described here, with the resident standing up more or less independently using the edge of the bed to pull himself up and support himself, with the help of the nurse reaching under his arms, was explained by another nurse in the home as ‘mobilization,’ as an activating measure. This means of organizing excretion, which usually takes place in the same manner, thus simultaneously serves to give the resident a certain amount of independence, or to have him practice it. It not only offers the resident support with excretion, but also acts as a relevant aspect of contemporary notions of activating nursing. The mobility offered by its rollers means the toilet chair can be used in different places; it becomes a ‘mobile toilet.’ This specific feature of the toilet chair allows both aspects of this professional care concept to be achieved at once, to support and mobilize the resident.
As the toilet chair can be employed flexibly, in different places, the resident’s bedroom in the scene described here can more or less be refitted as a bathroom, thanks to the mobile toilet chair, and used as such. The bedroom converted into a bathroom is something of a hybrid space, which clashes with the common understanding of the ‘smallest room’ as a place of total privacy. Further, previously unmentioned items are used to meet other expectations of contemporary nursing. Once the resident has sat down on the toilet chair, the nurse gives him an emergency buzzer and leaves the resident alone in his room. This fulfils the notions of discretion and privacy which dominate within society and nursing, as the resident is alone in his private bedroom, converted into a bathroom, during excretion, that is, left in peace.
At the same time, placing the emergency buzzer within reach appears to ensure that he can contact the nurse, thus ensuring the safety aspect which is frequently brought up in nursing — even if in the above scene the resident does not, in the end, use that opportunity. The fact that the resident sits on the toilet chair for about an hour without pressing the emergency buzzer indicates a mutual dependency. The nurse depends on the resident actually pressing it (which he appears to expect, as implied by his question about why the resident did not buzz). The resident, in turn, depends on the nurse coming (even if he does not buzz) and helping him out of the toilet chair, as he cannot get up from it and move to the wheelchair on his own, even when using the bed frame. The fact that the nurse only checks on the resident after an hour is an indication of rationalized work processes: while the resident does his business alone, the nurse goes about other jobs with other residents. The fact that the nurse does not push the toilet chair into the resident’s bathroom (or over the toilet, that is, the place where one might usually expect the excretion of excrement to take place) is another indicator that the nurse is cutting back on additional movements and time. The use of the toilet chair described above correlates with the increasing economization of care work, which is even redefining social understandings of the ‘smallest room’ (for example, moving it out of the bathroom and associating excretion with mobilization).
Nonetheless, in the above scene, certain normative notions of ‘appropriate’ excretion are also being fulfilled, even though it takes place in a different manner than usual: the bed frame creates a materially conveyed physical distance between the resident and the nurse. The latter just has to hoist the resident up under his arms to help him stand, which does not involve getting too close to him physically. [56] The gloves also help minimize physical proximity in that the nurse does not come into direct contact with the resident as he helps him cover his buttocks. [57] His genitals are not directly touched, thus preserving a certain amount of privacy. Another relevant object is the emergency buzzer, which acts as a promise that the nurse will remain available even after leaving the room. This might give both the resident and the nurse a feeling of certainty about the nurse’s potential availability and also allows the nurse to leave the situation, in turn leaving the patient undisturbed. This offers personal distance, rather than any great physical distance. Leaving the room seems to be part of an implicit protocol for maintaining a moment of privacy during excretion. [58] It can be seen that the use of the toilet chair as described here requires additional organization and additional items to create the ‘appropriate distance’ in order to maintain discretion. This ‘fine art’ of both maintaining the resident’s privacy (distance) on the one hand and promising safety (proximity) on the other corresponds with the material nature of the toilet chair, with its discreet and particularly sturdy design.
Teaching the Use of the Toilet Chair
Contemporary textbooks also raise both points: activating care and discretion during supported excretion using a toilet chair. It can be seen that the toilet chair creates an interactive framework for the nursing situation, as a professional nursing task. In the research on dirty work in nursing, this has been identified as a key method of dealing with private, perhaps even embarrassing and unpleasant touching and ‘dirty bodies.’
In more recent textbooks, in contrast with the books described in Chapter 3, there are separate sections on excretion, explicitly addressing the subject as an aspect of nursing and as culturally influenced. Thiemes Altenpflege [59] (Thieme’s Geriatric Nursing), for example, indicates that
Excretions are perceived as unpleasant or even disgusting in terms of their smell, appearance and nature. The excretory organs are in an area of the body which is hidden from sight. Most find it difficult to strip naked for daily washes of their private parts, or for the doctor’s examination. The embarrassment felt by the patient should not be injured or ignored, though we ourselves have learnt to overcome our inclinations. Even, or perhaps precisely, in this case, our respect for human dignity can be seen. [60]
Another textbook, Pflege heute [61] (“Nursing Today”), also offers the ‘practical tip’ of favoring toilet chairs over urinals, not only to encourage mobilization, but also to take feelings of embarrassment into account. Most textbooks therefore stress that those in need of care should be left alone during the process of excretion, whenever possible. [62]
Whilst earlier textbooks prioritize professional medical skills and knowledge of materials alongside patients’ welfare and physical safety (see Chapter 3), current textbooks emphasize activation, consideration for patients’ feelings of embarrassment, and the use of discretion towards them.
4_Conclusion
As we have shown in this article, material objects (or the nonhuman) are what aid carers in supporting people in cases where central human needs cannot be satisfied independently and the support of a carer is required. Our interdisciplinary research into the use of material objects from a current and a historical perspective has clearly shown the great extent to which professionals’ knowledge about objects and the ways they can be used can turn a situation which is difficult for both parties into something manageable. Social notions of discretion in view of the inevitable physical proximity and powerful touches which have to take place in nursing are manifested in objects. These objects have been adapted to the needs of patients and their specific situation. Interactions between people and material objects are of a very specific nature and differ from cases where people can use the toilet independently. Observing how material objects were and are used in practice thus shows us that the boundaries of the lavatory become redefined. For instance, the lavatory becomes positioned not in the bathroom but in the patient’s bed or bedroom, even if the excretion process took place with the support of other material objects (such as the emergency buzzer or the bed covers) as a discreet, solitary affair in accordance with the social conventions of excretion. By using material objects, the methods used by nurses and the ‘indiscreet’ touching they practiced were redefined as an aspect of professional nursing (as shown by the idea that the toilet chair mobilizes patients).
In conclusion, as demonstrated not only by us, but also by nurses, textbook authors and product manufacturers, linking or attaching expert and professional knowledge to material objects allows the ‘dirty body work’ of supported excretion within nursing to be interpreted and presented as professional and appropriate. This has various effects on patients’ bodies and how their bodies are treated. As it is the nurses who operate the objects related to the patients’ excretion, it is the nurses who have the decision-making powers and so take a determining role in this strongly experienced relation. The use of objects means that the individuals become part of a process which is guided and dominated by material objects. Patients are forced to submit to the workflow of the nursing process and are controlled by that process. Human bodies thus become part of an object-controlled process, even though supported excretion is a profoundly ‘human’ task which does in fact evoke an emotional response in human beings.
Generally, in the light of our investigations into material culture, it can be said that material objects can be accomplices, or have a complicity in supporting people’s needs. This is, however, somewhat ambivalent as, being material objects, they are caught up in cultural patterns of social order (related to dirt, feces, and dirty bodies). The material objects used in supported excretion are thus linked to a great extent with biased associations (of transgressing privacy, of crossing boundaries for instance) which, in turn, affects the way that nursing situations (supported excretion) take place, the notions of the body, age, dirt, gender, and so on that they produce and reproduce, and how they do so. Material objects help people to process emotions, but only to a certain degree, as their material form, their haptic and their additional symbolic meanings [63] always themselves produce emotions. As we have seen, not only people are required to wield power with the (chamber) pot, but also material objects. In our investigation, we were also able to show that material objects are associated with a wide range of aspects of cultural activity. For example, the discreet appearance of toilet chairs correlates with the idea which has prevailed since the bourgeois era that discretion should be maintained around processes of excretion. The toilet chair and its material appearance are symbolically imbued with discretion.
For various reasons (mainly economy of space), our work on the role of material objects in supported excretion in the setting of nursing was restricted to German-speaking countries. To find out more precisely what cultural status material objects have in nursing, rigorously intercultural investigative approaches are required of the kind currently being used, for example, in medical anthropology. However, one thing which is still lacking is a firmly object-based approach designed to carry out a more detailed intercultural, comparative investigation on the relationship of culture in a manner which is appropriate to the non-human. One desideratum would be for more of these aspects to be revealed in future, featuring intercultural comparison among other material objects. This would not only allow the topics which we have worked on to be extended further, but would also place the focus on objects’ cultural content once again.
_How to cite
Lucia Artner and Isabel Atzl. “Pot and Power: The Role of the Nonhuman in a Very Human Business.” On_Culture: The Open Journal for the Study of Culture 2 (2016). <http://geb.uni-giessen.de/geb/volltexte/2016/12355/>.
_Endnotes
- [1] This article was written as part of the research program “Die Pflege der Dinge: Die Bedeutung von Objekten in Geschichte und gegenwärtiger Praxis der Pflege” (Care and Things: Objects and their Significance in Past and Present Nursing Practice, see: <www.pflegederdinge.de>). The project on which this article is based is being funded by the Federal Ministry of Education and Research from February, 2014 until the end of January, 2017, funding code 01UO1317A. The authors bear responsibility for the content of this publication.
- [2] Tony Bennett and Patrick Joyce, eds., Material Powers: Cultural Studies, History and the Material Turn (Abingdon/New York: Routledge, 2010); Dan Hicks, “The Material-Cultural Turn: Event and Effect,” in The Oxford Handbook of Material Culture Studies, eds. Dan Hicks and Mary Carolyn Beaudry (Oxford: Oxford University Press, 2010), 25–98.
- [3] Mary Douglas, Purity and Danger: An Analysis of Concepts of Pollution and Taboo (London et al.: Routledge, 2002 [1966]); Sjaak van der Geest, “The Social Life of Faeces: System in the Dirt,” in Wildness and Sensation: An Anthropology of Sinister and Sensuous Realms, eds. Rob van Ginkel and Alex Strating (Amsterdam: Het Spinhuis, 2007), 381–397.
- [4] Jocalyn Lawler, Behind the Screens: Nursing, Somology, and the Problem of the Body (Sydney: Sydney University Press, 1991); Els van Dongen, “ ‘It Isn’t Something to Yodel About, but it Exists!’ Faeces, Nurses, Social Relations and Status within a Mental Hospital,” in Aging & Mental Health 5.3 (2001), 205–215.
- [5] Michel Foucault, The History of Sexuality: An Introduction. Vol. 1 (Pantheon Books: New York, 1978). Foucault’s concept of biopower relates more to the practices of nation states, of governance and political acts. But the idea that the biopower of a nation state is aiming at the concrete bodies of its citizens, to control their (bodily) behavior and to subjugate them so that they behave in a compliant way, can also be applied to the analysis of concrete nursing and care settings and the interactions taking place there between material objects and people.
- [6] Rachel Vanessa Lea, “The Performance of Control and the Control of Performance: Towards a Social Anthropology of Defecation” (PhD diss., Brunei University, London, 2001); Sjaak van der Geest, “Not Knowing about Defecation,” in On Knowing and Not Knowing in the Anthropology of Medicine, Roland Littlewood, ed. Roland Littlewood (Oxford: Berg, 2007), 75–86.
- [7] Sjaak van der Geest, “The Toilet: Dignity, Privacy and Care of Elderly People in Kwahu, Ghana,” in Ageing in Africa: Sociolinguistic and Anthropological Approaches, eds. Sinfree Makoni and Koen Stroeken (Aldershot: Ashgate, 2002), 227–244, here: 236.
- [8] Joseph B. Loudon, “Stools, Mansions & Syndromes,” in Rain 10 (1975), 1–5, here: 5.
- [9] Astrid Stölzle, Kriegskrankenpflege im Ersten Weltkrieg: Das Pflegepersonal der freiwilligen Krankenpflege in den Etappen des deutschen Kaiserreichs (Stuttgart: Franz Steiner Verlag, 2014).
- [10] Stölzle, Kriegskrankenpflege (cf. note 9), 56–96.
- [11] Douglas, Purity and Danger (cf. note 3), 2.
- [12] Van der Geest, “Not Knowing about Defecation” (cf. note 6).
- [13] Van der Geest, “Not Knowing about Defecation” (cf. note 6), 81.
- [14] Van der Geest, “Not Knowing about Defecation” (cf. note 6), 77.
- [15] Norbert Elias, Über den Prozess der Zivilisation: Soziogenetische und psychogenetische Untersuchungen I ( Suhrkamp: Frankfurt, Main, 1997), 272–285.
- [16] Van der Geest, “The Social Life of Faeces” (cf. note 3), 381–397.
- [17] John Gregory Bourke, Das Buch des Unrats (Frankfurt, Main: Eichborn, 1992); René Faber, Von Donnerbalken, Nachtvasen und Kunstfurzern: Eine vergnügliche Kulturgeschichte (Frankfurt, Main: Eichborn, 1994); Florian Werner, Dunkle Materie: Die Geschichte der Scheiße (München: Nagel & Kimche, 2011).
- [18] Michael Stolberg, Homo patiens: Krankheit und Körpererfahrung in der Frühen Neuzeit (Köln: Böhlau Verlag, 2003), 167–183.
- [19] Stolberg, Homo patiens (cf. note 18), 167.
- [20] Anne Marie Sandvoll, Ellen Karine Grov, Kjell Kristoffersen, and Solveig Hauge, “When Care Situations Evoke Difficult Emotions in Nursing Staff Members: An Ethnographic Study in Two Norwegian Nursing Homes,” in BMC Nursing 14.40 (2015), accessed November 16, 2016, <https://bmcnurs.biomedcentral.com/articles/10.1186/s12912-015-0093-7>; Stolberg, Homo patiens (cf. note 18), 170; Elias “Zivilisation” (cf. note 15).
- [21] Bettina Möllring, “Toiletten und Urinale für Frauen und Männer: Die Gestaltung von Sanitärobjekten und ihre Verwendung in öffentlichen und privaten Bereichen” (PhD diss., Universität der Künste, Berlin, 2003).
- [22] Lawler, Behind the Screens (cf. note 4); Van Dongen, “It Isn’t Something to Yodel About” (cf. note 4).
- [23] Van der Geest, “The Social Life of Faeces” (cf. note 3).
- [24] Based on Elias, “Zivilisation” (cf. note 15).
- [25] Mary Stewart, “ ‘I’m Just Going to Wash You Down’: Sanitizing the Vaginal Examination,” in Journal of Advanced Nursing, 51.6 (2005), 587–594, here: 588.
- [26] Stefan Dreßke,“Identität und Körper am Lebensende: Die Versorgung Sterbender im Krankenhaus und im Hospiz,” in Psychologie und Gesellschaftskritik 32 (2008), 2/3, 109–129.
- [27] Dreßke, “Identität und Körper” (cf. note 26), 115; English translation by the authors.
- [28] Van Dongen, “It Isn’t Something to Yodel About” (cf. note 4), 207.
- [29] Robert McMurray, “Embracing Dirt in Nursing Matters,” in Dirty Work: Concepts and Identities, eds. Ruth Simpson et al. (Basingstoke: Palgrave Macmillan, 2012) 126–142, here: 128.
- [30] Julia Twigg, Bathing: The Body and Community Care (London/New York: Routledge, 2000).
- [31] Stewart, “ ‘I’m Just Going to Wash You Down’ ” (cf. note 25), 588.
- [32] Stewart, “ ‘I’m Just Going to Wash You Down’ ” (cf. note 25), 588; also Twigg, Bathing (cf. note 30).
- [33] Ruth Simpson, Natasha Slutskaya, and Jason Hughes, “Gendering and Embodying Dirty Work: Men Managing Taint in the Context of Nursing Care,” in Dirty Work: Concepts and Identities, eds. Ruth Simpson et al. (Basingstoke: Palgrave Macmillan, 2012), 165–181, here: 168; Sharon C. Bolton, “Women’s Work, Dirty Work: The Gynaecology Nurse as ‘Other’,” in Gender Work and Organization, 12.2 (2005), 169–186.
- [34] Carol Wolkowitz, “The Social Relations of Body Work,” in Work, Employment and Society 16.3 (2002), 497–510.
- [35] Sandvoll et al., “When Care Situations Evoke Difficult Emotions” (cf. note 20).
- [36] The term “non-human actor” is often associated with the works of Bruno Latour and his interpretation of actor network theory (ANT). We do not disagree with the main premise of ANT of focusing on the agency, or potential agency, of material objects. However, we are more in accordance with material culture studies, which conceptualizes the role objects have in social interactions much more openly, emphasizing that objects might act but might also be ignored or forgotten and offering a much more differentiated idea of agency in general.
- [37] Van der Geest, “Not Knowing about Defecation” (cf. note 6), 78.
- [38] Lawler, Behind the Screens (cf. note 4); Irmgard Bauer, Die Privatsphäre der Patienten (Bern et al.: Verlag Hans Huber, 1996); Van Dongen, “It Isn’t Something to Yodel About,” (cf. note 4); Birgit Heimerl, “Choreographie der Entblößung: Geschlechterdifferenz und Personalität in der klinischen Praxis,” in Zeitschrift für Soziologie 35.5 (2006), 372–391; Sandvoll et al., “When Care Situations Evoke Difficult Emotions” (cf. note 20); Alexandra Hangl, “Ekel in der Krankenpflege: Orte, Praktiken und Funktionen,” in Bricolage: Innsbrucker Zeitschrift für Europäische Ethnologie 8 (2015), 83–104.
- [39] For further information on the research project “Care and Things” cf. note 1.
- [40] Johann Friedrich Dieffenbach, Anleitung zur Krankenwartung (Berlin: August Hirschwald Verlag, 1832).
- [41] Franz Christian Karl Krügelstein, Handbuch der allgemeinen Krankenpflege (Erfurt, 1807), 326.
- [42] Dieffenbach, Krankenwartung (cf. note 40), 104–106, 107–109.
- [43] Medizinalabteilung des Königlich Preußischen Ministeriums für Unterrichts- und Medizinalangelegenheiten, Krankenpflege-Lehrbuch (Berlin: August Hirschwald Verlag, 1910), 139; English translation by the authors.
- [44] Rudolf Salzwedel, Leitfaden der Krankenwartung: Zum Gebrauch für die Krankenwartschule des kgl. Charité-Krankenhauses (Berlin: August Hirschwald Verlag, 1896).
- [45] Salzwedel, Krankenwartung (cf. note 44), 71.
- [46] Dieffenbach, Krankenwartung (cf. note 40), 108.
- [47] Close stool: Edmund Alexander Parker, A Manual of Practical Hygiene 1 (1864), 620; necessary stool: F. Nicholls, Philosophical Transactions (Royal Soc.) 52 (1762), 267; night stool: Edmund Ronalds and Thomas Richardson, Knapp’s Chemical Technology (New York, 1854), 246.
- [48] Dieffenbach, Krankenwartung (cf. note 40), 26; English translation by the authors.
- [49] Rudolf Salzwedel, Handbuch der Krankenpflege: Zum Gebrauch für Krankenpflegeschulen sowie zum Selbstunterricht (August Hirschwald Verlag: Berlin 1909), 49; English translation by the authors.
- [50] Salzwedel, Handbuch der Krankenpflege (cf. note 49), 50–51; English translation by the authors.
- [51] Salzwedel, Handbuch der Krankenpflege (cf. note 49), 49; English translation by the authors.
- [52] Salzwedel, Handbuch der Krankenpflege (cf. note 49), 51.
- [53] See also Dreßke, “Identität und Körper am Lebensende” (cf. note 26).
- [54] “Die Pflege der Dinge: Die Bedeutung von Objekten in Geschichte und gegenwärtiger Praxis der Pflege” (cf. note 1).
- [55] Meant as “disciplined ways of seeing,” see Harold Garfinkel, Toward a Sociological Theory of Information (Boulder, CO.: Paradigm Books, 2008 [1952]).
- [56] This also apparently lightens the nurse’s physical burden, a subject which is mainly discussed within nursing in terms of work that is not stressing to the back.
- [57] By contrast, the nurses generally explained the use of disposable gloves for reasons of hygiene. They were said to protect the nurses against residents’ bacteria, etc. while on the other hand also protecting the residents against the nurses (their bacteria, etc.).
- [58] There were strong parallels between this and similarly structured situations of supported visits to the lavatory, in which residents sat on the toilet in the bathroom. Here, too, “enough” distance and discretion were mainly achieved by moving out of the room.
- [59] Ilka Köther, ed., Thiemes Altenpflege: Altenpflege professionell (Stuttgart: Thieme, 2007).
- [60] Köther, Thiemes Altenpflege (cf. note 59), 297–298; English translation by the authors.
- [61] Nicole Menche, ed., Pflege heute (München: Elsevier, 2007).
- [62] Susanne Schewior-Popp, Franz Sitzmann, and Lothar Ullrich, Thiemes Pflege: Das Lehrbuch für Pflegende in Ausbildung (Stuttgart: Thieme, 2009).
- [63] See Garfinkel, Toward a Sociological Theory of Information (cf. note 55); Gottfried Korff, “Sieben Fragen zu den Alltagsdingen,” in Alltagsdinge: Erkundungen der materiellen Kultur; Gudrun König (Tübingen: TVV, 2005), 29–42.